
Volume 25 Number 1
The Diabetic Foot Valley Project: bottom-up building of a community of practice for diabetic foot care in Tuscany
Alberto Piaggesi, Roberto Anichini, Fabio Baccetti, Cristiana Baggiore, Laura Bini, Ilaria Casadidio, Maria Calabrese, Antonio De Luca, Cecilia Fondelli, Chiara Goretti, Francesco Manetti, Matteo Monami, Margherita Occhipinti, Paola Orsini, Loredana Rizzo, Alessia Scatena and Graziano Di Cianni
Keywords guidelines, implementation, diabetic foot, good clinical practice, evidence-based medicine
For referencing Piaggesi A, et al. The Diabetic Foot Valley Project: bottom-up building of a community of practice for diabetic foot care in Tuscany. Journal of Wound Management. 2024;25(1):31-35.
DOI
10.35279/jowm2024.25.01.07
Submitted 15 December 2023
Accepted 13 February 2024
Abstract
To implement the regional guidelines on the management of diabetic foot (DF) into real practice, the diabetiologists working in the public diabetologic services of the Tuscany Region Health Service launched an bottom-up initiative called Diabetic Foot Valley, aiming in creating a community of practice for DF care in Tuscany, Italy.
The project, started in 2022 with three meetings dedicated to acute, sub-acute and chronic DF, respectively. The outcomes were articulated into amelioration projects (APs) which targeted the critical issues identified by the analysis performed inside the three meetings and which will be carried on in 2023 and 2024.
The outcomes of the APs will be evaluated at the end of their development and compared to the baseline, to evaluate the progress made. The APs already in place are those related to revascularisation, surgical management, local care and networking, with the designing and building of a dedicated electronic platform; others, like those dedicated to offloading, screening and prevention, rehabilitation and follow-up will start in 2024.
The project, endorsed by Regione Toscana and European Wound Management Association (EWMA), will serve as a pilot which can be a point of referral for similar experiences in other European countries for the implementation of the international guidelines on DF.
Background
Diabetic Foot Syndrome (DFS) is a complex multi-morbid condition affecting 25% of diabetic patients worldwide. It represents a clinical emergency because of its increasing incidence, severity, and progressiveness, with a trend to recur that reaches the striking rate of 98% at ten years follow up.1
In addition to being the first cause of non-traumatic lower limb/extremity amputation (LEA) in the world, exposing patients to a risk 20 times higher than the general population, DFS has a mortality rate of 60% in five years, comparable to that of the most aggressive cancer forms.2,3
In Italy diabetes mellitus has been recognised as a socially relevant disease, and a specific national law introduced in the late 1980s and implemented in the National Health Plan in 1999 (L115 of 16/03/1987), promoted the creation of a network of diabetologic services inside the National Health Service (NHS).4,5
Around 250,000 diabetic patients live in Tuscany, and among them 15,000 are affected by DFS. The problem had been recognised since the early 1990s, and many of the diabetological units in the region have set up some form of prevention and care for DFS.6
In 2003 the first regional law, promoted by diabetologists and enforced by the regional health authority, recognised the importance of DFS and set the organisation guidelines to provide an adequate level of care for this pathology, based on the model of the IWGDF guidelines (DLR 1304 of 09/12/2003)7.
In 2016, after a re-organisation of the Regional Health Service (RHS) in three macro-areas, a new edition of the Regional Law on DFS was released, to fit the DFS management inside the new model of the RHS (DLR 698 of 19/07/2016).8
Despite the premises, and the recognized expertise of some of the Tuscan clinicians, the implementation of the regional guidelines, did not happen, and the disparity of treatments, and outcomes between the different centres remained high.9,10
An analysis of the quality of outcomes in the RHS of Tuscany, made yearly by the MeS lab of Sant’Anna University (SSSUP), an independent auditor for RHS, revealed that the number of major amputations remained high and that wide variations in performances related to diabetic foot management, like revascularisation procedures, still characterised the scenario.11
The gap between the model design in the guidelines and the reality of DFS care in Tuscany became even more evident during the Covid-19 pandemic, when available resources were diverted to fight the emergency, leaving the other pathologies largely unattended; for DFS this meant an excess of lower limb amputations (+47%) and deaths (+62%) compared to pre-Covid years.12
The Diabetic Foot Valley Project
In order to overcome regional differences and to implement the already existing guidelines into clinical practice, the Tuscan diabetologists launched the Diabetic Foot Valley Project in July 2022, in an informal meeting in Pisa.
The aim was to create a community of practice that would include all the professionals — doctors (MDs), nurses (RNs), podologists (DPMs) — working in the regional healthcare system specialised in diabetes foot care, and organising them in an integrated network following the indications of the Regional Guidelines.
Firstly, an online survey was submitted to all the 15 Tuscan diabetic clinics to uniformly map the DF pathways, quantify the existing activities and identify the critical issues. The online questionnaires analysed several areas considered essential: availability of dedicated spaces and suitable equipment, screening, admissions and visits, revascularisation procedures, surgery, urgent pathways, follow-up and continuity of care. Consequently, a list of priorities was designed and three focus meetings organised, the first in Pisa on 3 December 2022, the second in Arezzo on 18 February 2023, and the third in Florence on 15 April 2023, respectively.
The three meetings, which were attended respectively by 62, 68 and 74 professionals. The first was 47.5% MDs, 26.2% DPMs and 26.3% RNs. The second was 47.6% MDs, 21.9% DPMs 30.5% RNs, and the third meeding was of 41% MDs, 19.7% DPMs, and 39.3% RNs. The RNs, MDs and DPMs were from the 15 diabetes clinics in Tuscany. They had the aim of comparing real-world clinical practice for DF with the Regional Guidelines, discussing the critical aspects, identifying barriers to best practices and promoting improvements.
The meetings were organised to maximize the direct involvement of the participants: after an initial plenary session, in which the results of the mapping were presented and the differences discussed, participants were divided in three focus groups which met separately in the second section of each meeting.
In the focus groups the critical aspects related to acute, sub-acute and chronic DF were discussed, and some amelioration projects (APs) were launched, to be developed over a 2 to 4 year span, to connect the level of assistance to the model indicated by the guidelines. The amelioration projects identified by the focus groups in each of the three meetings were related to:
- Improvement of the revascularisation pathway, the management of urgent cases and the management of Charcot patients with Acute DF;
- Local care, the use of negative pressure wound therapy (NPWT), and integration between hospitals and the community for the sub-acute DF;
- Primary prevention and the early diagnosis, the timely referral of cases and the rehabilitation of cases for chronic DF.
Moreover, an amelioration project interesting all the phases of the management of DF was decided, i.e. the realization and implementation of a dedicated operational software and electronic database to be shared by alla the centers of the DFV community of practice.
All APs aimed at upgrading and standardizing the methods according to the indications of the Regional Guidelines; one of the APs, indicated as a priority, was the realisation of a dedicated Regional Electronic Operative Instrument, which should not only act as a Case Report Form (CRF), but also as a database of both clinical, organization and econometric information.
The results will be evaluated at the end of the APs and compared with the data collected before their development, according to the scheme reported in Figure 1.
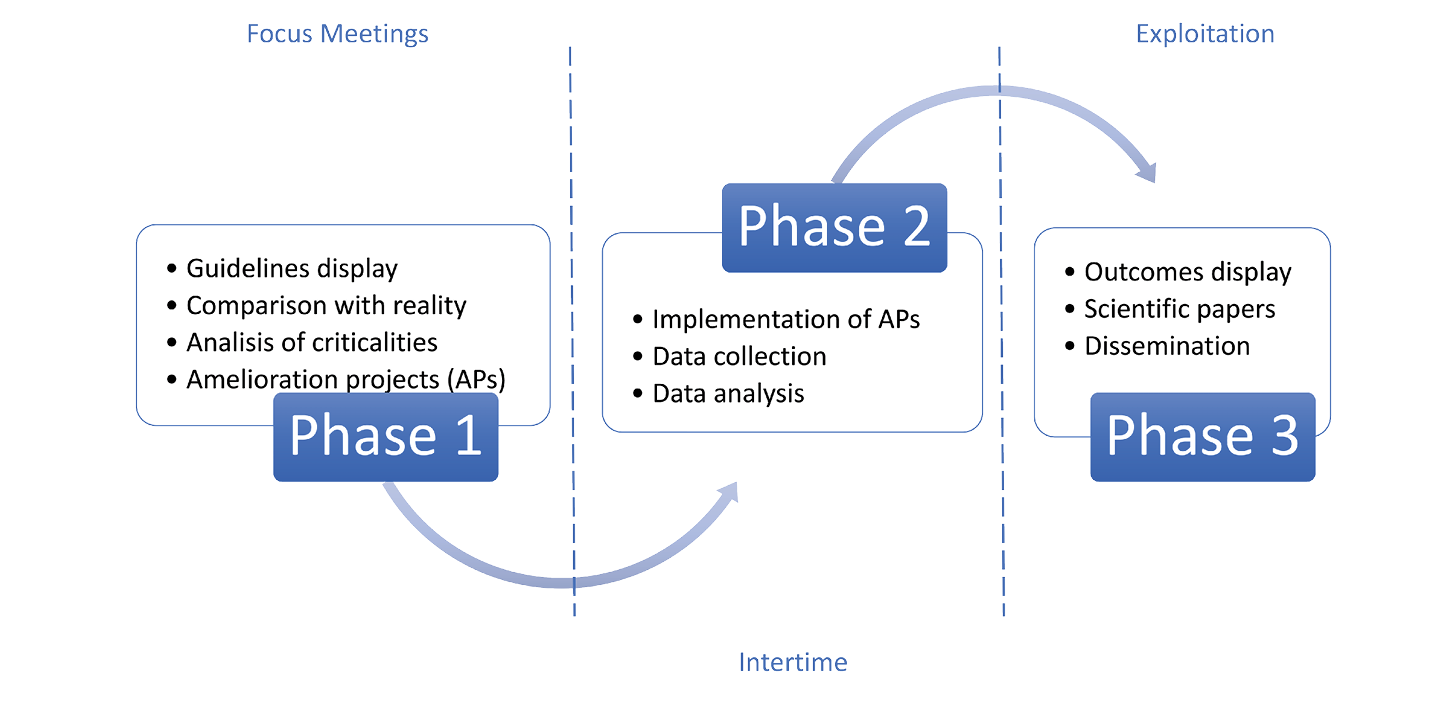
Figure 1. The general scheme of the Diabetic Foot Valley Project
Expected Outcomes
Although the general scheme of the project does not yet give precise indications of the outcomes, as these will arise from the AP structures and their targets, still some preliminary forecast can be made.
The APs deployment and analysis stages are designed so that results will be available between 2 and 4 years after commencement, depending on the complexity of the projects and on whether the information can be collected from the centers in a timely manner.
For this purpose, a new regional database and operational software for the management of DFS patients in the public diabetologic network will be designed, implemented and financed by Tuscany Region as part of the National Plan for Resilience and Recovery (PNRR).13
This will be the AP #1 and will serve both as a connecting system between the different centers of the network and as a dataset in which all the information on the patients will be put, rendering it available for analysis of progression of the other APs.
The other APs will focus on the criticalities that emerged in the focus groups and their outcomes will depend on the nature of the critical items and the nature of the projects; some of them have already been set and are related to the quality and quantity of interventional procedures, in terms of revascularisation and infection management, and they will be most likely monitored by indicators that reflect not only the final outcome (i.e. healing, amputation, death), but also by intermediate outcomes, like delay of referral, number of procedures per patient, recurrences, and complications.
This approach came directly from the interpretation of DFS as a chronic-remitting-recurring pathology, rather than as an acute one; an idea shared by all the participants in the project, who agreed on the design and who are each involved in a number of APs, each targeting one aspect of the disease.
The Role of EWMA
Diabetic Foot Valley Project is endorsed by EWMA, as it is seen as a European model for improving patient outcomes, which can potentially be transferred to other regions and pathologies.
In addition, it can produce information on a numerically significant group of patients managed homogeneously in a welfare-based health care system. This could be important, not only to collect clinical and scientific data but also, to evaluate the efficacy and efficiency of the system from a health–economic and organisational point of view.
As a positive side effect, realising an integrated network of centers treating DF may attract the industry to conduct clinical trials, serving as a one-stop shop for companies. This is — from EWMA’s perspective — an important contribution to attracting and maintaining clinical trials in Europe. Showing progress on this front, two clinical studies have already started in some of the Centers of DFV.
Institutional Involvement
The Diabetic Foot Valley Tuscany has already been presented to the General Director of the Health Authority of Tuscany, who endorsed it and authorised the development of the Regional Electronic Operative Instrument Under the responsibility of the Regional Electronic Data Management Department as a first step for finalising the project.
Steps Ahead
After the first phase, in which the APs are being developed (five of them have already been set), the second phase will take place over the next two years, at the end of which results before and after will be compared to assess the efficacy of the intervention, from both on clinical and organisational sides.
Each AP will be designed as a prospective interventional study, according to the principles of good clinical research practice and with regard to the privacy and dignity of the patients, according to current laws and regulations.14,15
The results of each study will be analysed with a scientifically sound methodology, and submitted by the focus group that suggested it to a peer-reviewed journal. The results will also be discussed and presented at a dedicated congress focused on the project.
The same results will be then presented at EWMA scientific meetings, to promote a discussion on DF management in Europe and to propose a methodology to improve the organisation of care on this so-far neglected pathology.
Conclusions
The Diabetic Foot Valley Project is a bottom-up initiative, started in Tuscany, aimed at creating a community of health professionals involved in the care of the patients affected by DFS, improving both prevention, early diagnosis and treatment by implementing the clinical and organisational guidelines into a clinical multidisciplinary network inside the Regional Health Service of Tuscany. The amelioration projects planned by the focus groups will target the criticalities highlighted by an analysis of the existing situation and their efficacy will be evaluated by a comparison of clinical and organisational parameters before and after the intervention and will be discussed and published as a result of the whole community of care. Possibly Dibetic Foot Valley may serve as a model to apply in other Regions or Countries in Europe, under the auspices, and with the support, of EWMA.
Acknowledgments
The authors acknowledge the technical and logistic support of Ing. Simone Barbagallo, of Hippocrates Research, and of Dr Peter Frank, of CAP-partner throughout the whole development of the project.
Contribution of the Authors
AP designed the Study, wrote and revised the manuscript; RA, FB, CB, LB, IC, MC, ADL, CF, CG, FM, MM, MO, PO, LR, AS, GDC participated in the design of the study, and discussed and revised the manuscript.
Disclosure
All the authors declare to have no duality of interests in relation to their role in the writing and editing of the present article.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
Funding for this project was provided by EWMA and Pisa International Foot Course
Author(s)
Alberto Piaggesi*1 MD, Roberto Anichini2 MD, Fabio Baccetti3 MD, Cristiana Baggiore4 MD, Laura Bini5 MD, Ilaria Casadidio6 MD, Maria Calabrese7 MD, Antonio De Luca8 MD, Cecilia Fondelli9 MD, Chiara Goretti1 MD, Francesco Manetti10 MD, Matteo Monami11 MD, Margherita Occhipinti12 MD, Paola Orsini13 MD, Loredana Rizzo14 MD, Alessia Scatena15 MD and Graziano Di Cianni16 MD, for the Diabetic Foot Valley Tuscany community of practice**
1Diabetic Foot Section, University Hospital of Pisa, Italy
2Centro Aziendale Podopatia Diabetica USL Toscana Centro, Pistoia, Italy
3Operative Unit of Diabetes and Metabolic Disease, Carrara, Italy
4Centro Aziendale Podopatia Diabetica USL Toscana Centro, Firenze, Italy
5Diabetology Unit Hospital of Pontedera, Italy
6Diabetology Unit Hospital of Lucca, Italy
7Centro Aziendale Podopatia Diabetica USL Toscana Centro, Prato, Italy
8Centro Aziendale Podopatia Diabetica USL Toscana Centro, Empoli, Italy
9Diabetes Unit, University of Siena, Siena, Italy
10Centro Aziendale Podopatia Diabetica USL Toscana Centro, Firenze, Italy
11Diabetic Foot Unit – Azienda-Ospedaliero Universitaria Careggi, Firenze, Italy
12UOS Diabetologia Versilia Hospital, Viareggio, Italy
13UOC Diabetologia e Malattie del Metabolismo, Livorno, Italy
14Diabetes and Metabolic Diseases Unit; Misericordia Hospital of Grosseto, Italy
15Diabetology Unit, San Donato Hospital Arezzo, Italy
16Diabetology Complex Unity, North West Tuscany, Italy
* See Appendix 1 for the complete list of participants in the Diabetic Foot Valley Tuscany project
*Corresponding author email alberto.piaggesi@med.unipi.it
References
- Armstrong DG, Boulton AJM, Bus SA. Diabetic foot ulcers and their recurrence. N Engl J Med. 2017 Jun 15;376(24):2367–2375. doi: 10.1056/NEJMra1615439. PMID: 28614678
- Armstrong DG, Tan TW, Boulton AJM, Bus SA. Diabetic Foot Ulcers: A Review. JAMA. 2023 Jul 3;330(1):62–75. doi: 10.1001/jama.2023.10578. PMID: 37395769
- Armstrong DG, Swerdlow MA, Armstrong AA, Conte MS, Padula WV, Bus SA. Five year mortality and direct costs of care for people with diabetic foot complications are comparable to cancer. J Foot Ankle Res. 2020 Mar 24;13(1):16. doi: 10.1186/s13047-020-00383-2. PMID: 32209136; PMCID: PMC7092527
- https://www.gazzettaufficiale.it/eli/id/1987/03/26/087U0115/sg (cited 2023 October 4)
- https://www.gazzettaufficiale.it/eli/id/1999/07/16/099G0301/sg (cited 2023 October 4)
- https://www.siditalia.it/informazione/dove-curarsi/71-informazione/dove-curarsi/308-toscana (cited 2023 October 4)
- Bollettino Ufficiale Regione Toscana, DLR 1304 del 09/12/2003 “Linee guida organizzative per la gestione del piede diabetico”. (cited 2023 October 4)
- Bollettino Ufficiale Regione Toscana, DLR 698 del 19/07/2016 “Percorso diagnostico-terapeutico assistenziale della persona affetta da Piede Diabetico: Linee di indirizzo regionali”. (cited 2023 October 4)
- Piaggesi A, Ferraresi R, Gargiulo M. The Elephant in the Room. Int J Low Extrem Wounds. 2023 Jul 31:15347346231191229. Epub ahead of print.
- Nuti S, Bini B, Ruggieri TG, Piaggesi A, Ricci L. Bridging the gap between theory and practice in integrated care: The case of the Diabetic Foot Pathway in Tuscany. Int J Integr Care. 2016 May 24;16(2):9.
- Piaggesi A, Coppelli A, Goretti C, Iacopi E, Mattaliano C. Do you want to organize a multidisciplinary diabetic foot clinic? We can help. Int J Low Extrem Wounds. 2014 Dec;13(4):363-70. doi: 10.1177/1534734614545876. Epub 2014 Aug 14. PMID: 25123372
- .Iacopi E, Pieruzzi L, Goretti C, Piaggesi A. I fear COVID but diabetic foot (DF) is worse: a survey on patients’ perception of a telemedicine service for DF during lockdown. Acta Diabetol. 2021 May;58(5):587–593.
- https://www.epicentro.iss.it/politiche_sanitarie/pne-2020, Istituto Superiore di Sanità, Programma Nazionale Esiti 2020. (cited 2023 October 4).
- https://pnrr.toscana.it/-/missione-6-sanita-territoriale-innovazione-del-servizio-sanitario, (cited 2023 February 10).
- Commission Directive 2005/28/EC of 8 April 2005 laying down principles and detailed guidelines for good clinical practice as regards investigational medicinal products for human use, as well as the requirements for authorisation of the manufacturing or importation of such products. European Community, Brussels, 2005. 5.
- Council of Europe. Convention for the Protection of Human Rights and Dignity of the Human Being with regard to the Application of Biology and Medicine: Convention on Human Rights and Biomedicine, (Oviedo Convention), European Treaty Series No 164, Strasbourg, 1997.
Appendix 1
Complete list of the participants to the Diabetic Foot Valley Project
Abbruzzese Lorenza DPM (Pisa), Achilli Valeria DPM (Piombino), Amato Elisa DPM (Pisa), Ambrosini Nobili Laura DPM (Pisa), Amendola Carmelina RN (Prato), Amendolia Michela DPM (Livorno), Anichini Roberto MD (Pistoia), Apicella Matteo DPM (Arezzo), Baccetti Fabio MD (Carrara), Baggiore Cristiana MD (Firenze), Banchellini Elisa DPM (Lido di Camaiore), Barbaro Valeria MD (Firenze), Barnini Genny DPM (Empoli), Baronti Walter DM (Grosseto), Bastarelli Eleonora RN (Firenze), Becherini Roberto MD (Pistoia), Bernini Arianna DPM (Empoli), Bertoli Stefania MD (Camaiore), Bini Carlotta RN (Firenze), Butini Sofia RN (Arezzo), Cacioli Elisabetta RN (Grosseto), Calabrese Maria MD (Prato), Cameron Smith Michela MD (Firenze), Casadidio Ilaria DPM (Lucca), Chelli Cristina RN (Grosseto), Colombi Claudia MD (Firenze), Costa Alessandro DPM (Lido di Camaiore), Cossu Cristina RN (Grosseto), Crisci Isabella MD (Viareggio), Cuccuru Ilaria DPM (Lucca), De Gennaro Giovanni MD (Grosseto), De Gregorio Simona DPM (Pontedera), De Luca Antonio MD Empoli, Del Bianco Elisa RN (Lucca), Della Valentina Simone DPM (Pisa), Desideri Arianna DPM (Lucca), Di Carlo Alberto MD (Lucca), Faenzi Manuela RN (Firenze), Fanelli Stefania PsyD (Arezzo), Fondelli Cecilia MD (Siena), Giangreco Francesco MD (Pisa), Golini Romina RN (Arezzo), Goretti Chiara MD (Pisa), Gori Roberta RN Firenze, Iacopi Elisabetta MD (Pisa), Ieri Matteo DPM (Firenze), Lacaria Emilia DPM (Livorno), Landini Cristina RN (Bordo San Lorenzo), Lazzeri Andrea DPM (Firenze), Lencioni Cristina MD (Lucca), Leporati Elisa MD (Pisa), Leva Teresa RN (Lucca), Lorenzetti Monica MD (Prato), Luppichini Linda DPM (Firenze), Magi Silvia DPM (Arezzo), Maionchi Dino MD (Lucca), Manetti Francesco MD (Bagno a Ripoli), Mantuano Michele MD (Arezzo), Marinelli Elisa RN (Arezzo), Marsocci Angela (MD) Prato, Martinez Carmela RN (Arezzo), Mattesimi Mary RN (Arezzo), Monami Matteo MD (Firenze), Musco Marco DPM (Firenze), Neri Barbara DPM (Prato), Nigro Rosa RN (Arezzo), Nreu Besmir DPM (Firenze), Occhipinti Margherita MD(Lido di Camaiore), Orsini Paola MD (Livorno), Palladino Lavinia (Pisa), Parra Cecilia DPM (Lucca), Piacentini Marzia RN (Lucca), Piaggesi Alberto MD (Pisa), Piccini Valentina MD (Empoli), Pieruzzi Letizia MD (Pisa), Polloni Catia RN (Grosseto), Postiglione Gabriella RN (Prato), Ragghianti Benedetta MD (Firenze), Ranchelli Anna (Arezzo), Riitano Nicola DPM (Pisa), Rizzo Loredana MD (Grosseto), Rabuchia Anxhela DPM (Prato), Russo Chiara RN (Lucca), Sabatini Giovanna DPM (Firenze), Elisabetta Salutini MD (Pistoia), Sambuco Laura MD (Grosseto), Sandroni Sara RN (Arezzo), Sarzanini Maheva DPM (Carrara), Scatena Alessia MD (Arezzo), Serantoni Simone MD (Prato), Silverii Giovanni Antonio MD (Borgo San Lorenzo), Simi Barbara RN (Grosseto), Telleschi Massimiliano RN (Empoli), Trapani Edoardo DPM (Grosseto), Valdambrini Cristiana RN (Grosseto), Vannacci Serena RN (Grosseto), Viti Secondina MD (Pescia).
Appendix 2

Photo of the participants in the Diabetic Foot Valley project, taken in Florence on 15 April 2023.