

Volume 29 Number 1
Identifying contributing factors to tracheostomy stoma breakdown: a retrospective audit in a single adult intensive care unit
Karyn Heineger, Kathy Hocking, Nanette Paxman, Stacey Llewellyn, Anita Pelecanos and Fiona Coyer
Keywords skin injury, critical care, tracheostomy
For referencing Heineger K et al. Identifying contributing factors to tracheostomy stoma breakdown: a retrospective audit in a single adult intensive care unit. Wound Practice and Research 2021; 29(1):10-17
DOI https://doi.org/10.33235/wpr.29.1.10-17
Abstract
Introduction Tracheostomies are a common adjunct to therapy for critically ill patients in the intensive care unit (ICU). This study sought to identify the incidence of, and demographic, clinical and care process factors related to, tracheostomy-related skin injuries (TRSI) in ICU patients.
Methods Conducted in a 36-bed ICU of an Australian metropolitan tertiary referral acute care health facility, this study employed a retrospective review of patient records between February 2015 and December 2016 for patients who had a tracheostomy inserted during an ICU admission. Records were reviewed for the patient’s admission or a 20-day observation period, whichever was shorter.
Results Of the 102 patients included, 66 were male (64.7%) and their mean age was 50 years (SD=18.3). Of these patients, 23 (22.5%) developed a TRSI. No association was found between patient characteristics, tracheostomy insertion method and the development of a TRSI; however, the use of non-adjustable flange tubes was associated with the development of TRSI (p=0.023). Omissions in nursing documentation of care processes for tracheostomies were observed.
Conclusion This study addressed a specific medical device, the tracheostomy tube, providing evidence of TRSI occurrence in the ICU setting. Although no common demographic, clinical nor care process factors were associated with TRSI development, findings from this study highlight a deficiency in nursing documentation.
Background
Development of medical device-related pressure injuries (MDRPI) results from the use of devices for therapeutic or diagnostic purposes and are well recognised as separate from traditional pressure injuries (PI)1. Studies by Barakat-Johnson et al.2,3, Cooper et al.4 and Hanonu & Karadag5 found the development of a MDRPI can be difficult to prevent when the device is essential to a patient’s treatment and that patients in the intensive care unit (ICU) are a vulnerable patient group due to the high use of medical devices in their care. Currently there is little information relating to the type of injury caused by different devices in the critical ill patient population6. This study examines tracheostomy tubes and skin injuries related to this specific medical device – tracheostomy-related skin injuries (TRSI).
Critically ill patients in the ICU often require multiple devices for monitoring of physiologic parameters whilst receiving medical treatment5. The most common risk factor for developing a MDRPI has been reported as patients with impaired sensory perception, that is, ICU patients where therapeutic and pharmacological management of their critical illness may limit their sensory perception and ability to inform staff of discomfort or pain. The high use of medical devices in ICU, combined with the known risk factors of pressure, shear and altered skin microclimate, create a formula for the development of MDRPI within the ICU patient cohort7. Although not an exhaustive list, other contributing factors amongst the ICU patient group include prolonged immobility, reduced sensory perception due to paralysis/sedation, hypoxia requiring mechanical ventilation, haemodynamic instability resulting in poor tissue perfusion, and the use of vasopressors8.
One commonly used medical device in ICU is a tracheostomy tube. A tracheostomy creates an artificial opening or stoma into the trachea and is either performed surgically or by percutaneous dilation techniques (PDT). The stoma is kept patent by inserting a tube, generally made of thermosensitive polyvinyl chloride, through the opening9. Temporary tracheostomy is increasingly used earlier in the management of the general ICU population with the following three factors contributing to this; a reduction in the need for sedation; the promotion of earlier ventilator weaning and mobilisation; and the uptake of PDT, a quick and relatively safe procedure which can be performed at the bedside by ICU physicians10. The four general indications for a tracheostomy are: prolonged mechanical ventilation; airway patency; airway protection; and secretion management11. Peristomal skin breakdown or PI development is a known complication of tracheostomy11.
Loss of skin integrity related to a tracheostomy is multifactorial and even the type of tracheostomy tube used may influence the risk of developing a MDRPI12. For mechanically ventilated patients with a tracheostomy, downward traction of the tracheostomy tube caused by the weight of ventilator tubing produces pressure along the inferior margin of the stoma11. This downward torque can also contribute to the tracheostomy flange causing pressure over the bony prominences of the clavicles at the sternal junction4. Excessive moisture from leakage of respiratory secretions and/or saliva pooled above the cuff leads to overhydration and changes in skin microclimate which can lead to an increased risk of tissue breakdown7. These secretions may collect along the lower margin of the tracheostomy stoma, soak tracheostomy dressings, and promote maceration of the skin4. Pressure from the tracheostomy tube against the mucosal lining of the trachea can also cause pressure injuries to the mucosal lining1. As the trachea is essentially anatomically straight, the curved tracheostomy tube may not conform to the shape of the trachea which can lead to compression of the membranous/mucosal lining of the trachea13. This can then lead to increased leakage of respiratory secretions and/or saliva due to enlargement of the tracheal stoma.
MDRPIs differ from other PIs as they generally conform to the pattern or shape of the device4 and it is therefore the direct or indirect interaction of the device with the skin as opposed to body weight causing the injury7. Skin integrity loss or injury attributed to a tracheostomy does not conform to the definition of a MDRPI. This is because TRSI can be a mixture of mucosal and skin injuries related to a combination of pressure, the medical device being placed through a surgical wound, and from moisture, either from humidification or perspiration between the tracheostomy flange and skin, or from leaked saliva and/or respiratory secretions from the stoma12.
Evidence pertaining to tracheostomy-related PI is scant. One study by O’Toole et al.14 conducted in patients with only surgical tracheostomies identified a PI incidence pre-intervention of 10.9% (20/183) and an incidence of 1.3% (2/155) post-implementation of a PI prevention bundle. However, this study is limited by a lack of clear definitions of PI around a stomal site and a sample of surgical tracheostomy insertions only.
At our study site tracheostomy insertions have become part of standard practice when indicated for specific patients in the ICU. In February 2015, the Tracheostomy Management Service (TMS) commenced operation. This is a multidisciplinary team consisting of a medical staff specialist, clinical nurse consultant (CNC), physiotherapist and speech pathologist. This team supports ward staff in managing patients discharged from ICU with a tracheostomy, excluding those under the direct care of the Ear, Nose and Throat medical staff specialists. Part of the TMS clinical role includes regular tracheostomy stoma skin inspections, development of stoma care plans, and ensuring nursing staff report tracheostomy stoma skin injuries using the hospital adverse event reporting system.
An anecdotal increase in ICU TRSI was observed by the TMS CNC and required further investigation. Current literature approximates 10% of all PIs are device-related; however, there is a paucity of literature examining TRSI4,15.
Aims
The aims of this study were to two-fold – to identify the incidence of TRSI in patients in the ICU and to identify common demographic, clinical and care process factors amongst patients who developed a TRSI or stomal breakdown.
Study design
The study used a retrospective chart review design.
Subjects/patients
All adult patients admitted to the ICU from February 2015 until end-December 2016 who had a tracheostomy inserted, either surgical or percutaneous, during their admission were included. The commencement date was chosen as this was the date of commencement of the TMS at this facility. Patients under the direct care of Ear Nose and Throat team were excluded as the TMS was not involved in their care nor follow-up.
Setting
The setting was the 36-bed ICU of a metropolitan tertiary referral acute care health facility in Brisbane, Australia. The ICU admits general medical, surgical and trauma patients with specialities including burn, neurosurgery and trauma emergencies. The ICU admits approximately 2,400 patients per year with an admission illness severity mean score of 18 as determined by the Acute Physiology and Chronic Health Evaluation (APACHE) II16,17. The mean length of patient stay is 3.6 days. Medical management is provided by specialist intensive care physicians. Patients are cared for at a ratio of one nurse per mechanically ventilated patient or one nurse to two non-mechanically ventilated patients.
Measurements
Patient clinical information was retrieved from the ICU electronic clinical information system. All patient data was provided to the researchers in re-identifiable form to allow cross checking of clinical information system charting and notes. The first author reviewed all patient notes retrieved from clinical information system and cross-checked these for accuracy. Data was collected in 2-day blocks from the time of tracheostomy insertion for the patient’s admission or a 20-day observation period, whichever was shorter. Data comprised of patient demographic and clinical characteristics including ICU discharge and tracheostomy insertion procedural features. Data were collected related to medication administration and daily tracheostomy processes of care including stoma dressing replacement, tracheostomy suctioning, presence of stomal oedema, other skin site PIs, stage of PIs and enteral feeding. Tracheostomy suctioning frequency was defined as the highest frequency of suctioning occurring over the patient’s ICU stay. Correct cares administration was defined as the proportion of patients with correct processes of cares administered for each 2-day period. Cares administration was considered correct if the number of ordered cares as per the hospital-wide procedure for tracheostomy care in the 2-day period were equivalent to the documented cares, with both less or more cares administered than what was ordered considered incorrect. Cares documentation was defined as the percentage of days for which cares were documented over the total time a patient was observed.
Procedures
This project was approved by the Hospital Human Research Ethics Committee (HREC/17/QRBW/20). Following ethical and site governance approvals, the principal investigator identified all patients who had a tracheostomy in the ICU through the TMS master list and reviewed all relevant patient records from the ICU clinical information system. A master log to de-identify patients was created and all patients were assigned a unique study number. ICU medical staff specialists who performed tracheostomy procedures were allocated a code number for de-identification purposes. Data collected was stored electronically on a password-protected computer database held by the principal investigator.
Outcome measure
The outcome measure was the development of any TRSI, defined as an adverse change to the integrity of the tracheostomy stoma and/or surrounding peristomal skin. This differs to a PI which is defined as “localised injury to the skin and/or underlying tissue usually over a bony prominence, as a result of pressure, or pressure in combination with shear”1.
TRSI may be evidenced as an area of tissue loss, ranging from superficial epidermal loss to mid to deep dermal loss generally occurring in a crescent shape with even edges along the inferior margin of the stoma. The area of tissue loss can have the appearance of a thin layer of yellow devitalised tissue or at other times it can present as pale pink. The stomal margins may be macerated due to excess moisture from saliva and/or respiratory secretions (Figure 1). Moisture causing maceration also affects skin integrity which may make epidermal layers more susceptible to PI5.

Figure 1. Tracheostomy stoma showing maceration from moisture
In some cases, hypergranulation tissue may be present either as a direct result from tube irritation of stomal margins or excess moisture or a combination of both, or can occur during the healing process. The wound edges are generally flat and gently slope to the base of the wound. PDT are associated with increased technical difficulties when compared to surgical tracheostomy18. Skin damage or tearing can also occur during the actual dilatation process, leaving uneven skin edges and exposing underlying tissue. Figure 2 illustrates the uneven V-shaped skin tear that can happen during a percutaneous dilatational insertion which differs from the typical even crescent shape stomal margin (Figure 1).

Figure 2. Tracheostomy stoma showing V-shaped margin
TRSI were not staged using the recognised PI stages1 as it was difficult to define aetiology of the wound given multiple causative factors were often involved. This decision was endorsed by the facility’s Skin Safety Committee and supported by recent international guidelines1 recommending maceration, excoriation or skin tears should not be described as stage 2 PI.
Analysis
Data were analysed using SPSS version 23 (IBM Corp., Armonk, NY). Categorical variables were summarised using frequency and percentage and continuous variables by mean and standard deviation (SD) for normally distributed variables or median and interquartile range (IQR) for non-normally distributed variables. Associations with time to TRSI development for categorical demographic, comorbidities, tracheostomy, PI variables of interest were assessed using Kaplan-Meier analysis and compared using the Log-rank test. For continuous variables, associations with time to TRSI development were assessed using Cox proportional regression. Statistical significance was set at p<0.05.
Results
There were 102 patients included who were admitted to ICU and had a tracheostomy inserted during their admission between February 2015 and December 2016. The majority of patients were male (64.7%, 66/102) with a mean age of 50 years (SD=18.3). Of these patients, 23 (22.5%) developed a TRSI during their ICU admission. Table 1 summarises patient characteristics. Table 2 summarises the factors associated with tracheostomy insertion of all included patients. Table 3 summarises the post-tracheostomy insertion characteristics and clinical care processes in the audit population during ICU stay and highlights the low percentage of correct care administered.
Table 1. Patient characteristics
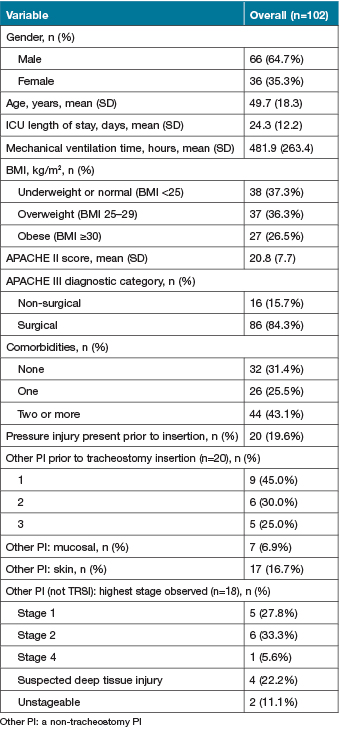
Table 2. Tracheostomy tube insertion characteristics
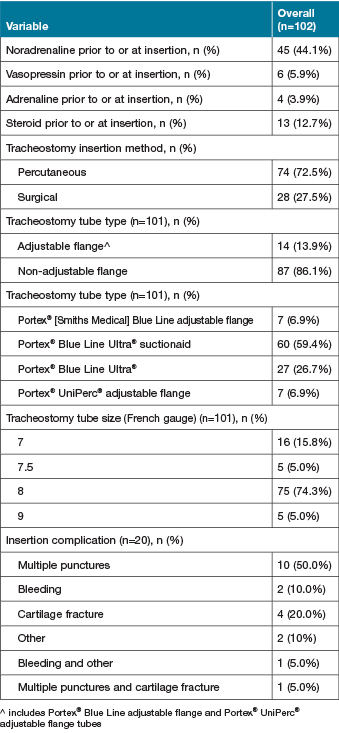
Table 3. Day 2 to Day 20 post-tracheostomy insertion: patient characteristics and clinical care processes

A number of patients were discharged from ICU prior to either TRSI development or before the end of the 20-day observation period. Patients who were discharged from ICU prior to the full 20 days of observation were marked as censored and their data collection was ceased at the time at which they were discharged. Censoring of data occurred as the observed value of some variables was only partially known, i.e. patients were discharged prior to completion of the 20-day observation period post-tracheostomy insertion therefore information about time to TRSI development was incomplete. Patients who remained in ICU for the full 20 days were censored and data collection was completed irrespective of TRSI development or not.
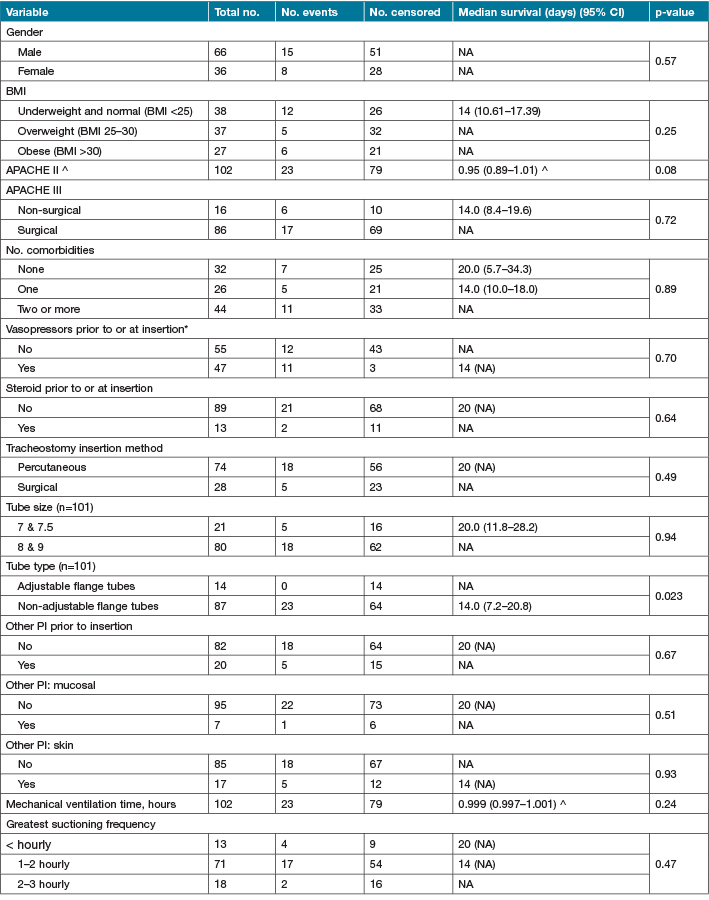
Kaplan-Meier analyses for the association of factors of clinical interest with TRSI development are shown in Table 4. In many cases the confidence intervals or the median survival estimate was unable to be determined due to insufficient events. The only factor found to be significantly associated with time to TRSI development was tube type (p=0.023). There were 23 TRSI that developed in patients who had non-adjustable flange tubes (65 censored), whilst there were no patients who developed a TRSI in patients who had adjustable flange tubes (14 censored). The median survival time to development of a TRSI was 14 days (95% CI: 7.2–20.8 days) for patients with non-adjustable flange tubes. The median survival time to the development of TRSI in patients with adjustable flange tubes was not defined as all data were censored; however, the median survival time was greater than 20 days.
Table 4. Kaplan-Meier survival estimates of time to TRSI development for categorical variables and Cox regression estimates for continuous variables
Discussion
Of the 102 patients who received a tracheostomy in ICU, 73% had a percutaneous insertion and a standard Portex® Blue Line Ultra® adult tracheostomy tube (non-adjustable flange), with or without suctionaid port was inserted in 86% of these patients. The use of a non-adjustable flange tube may be associated with a higher incidence of TRSI due to its more frequent use, leading to greater numbers of this tube type in this study. The use of an adjustable flange tube with its increased length of tube protruding from the neck creates a longer lever arm and increased potential for downward pressure/traction at the stoma site which may potentially increase the risk of TRSI. However, due to low study numbers, the association between this tube type and TRSI cannot be accurately reported on.
We found no evidence of an association between methods of insertion, administration of inotropes prior to or at the time of tracheostomy insertion, and the development of a TRSI. Further, no specific patient characteristics could be established as contributing to the development of a TRSI. The literature suggests all patients with a medical device are at risk for a device-related PI and no unique risk factors have been found that allow identification of high-risk patients19,7.
Currently, there is no unique predictive tool for assessing risk for development of a TRSI. Therefore, clinical judgement and visual skin inspections are required to assess for MDRPI; given this, some may go unrecognised or recorded20. A study in 2019 by Sankovich et al.21 demonstrated variations in staging of PI by nurses which was related to variability in assessment skills and knowledge deficits. This finding applied in the context of TRSI could mean that TRSI is potentially more difficult to diagnose. At our study site, a dedicated TMS CNC, a senior clinician with well-honed clinical assessment and judgement skills, increases the potential for early identification and management of TRSI.
Appropriate peristomal skin care, and application of a dressing to manage moisture and off-load pressure are interventions designed to reduce the risk of MDRPI22. Regular skin inspections and keeping the site as dry as possible, combined with positioning the tube in the neutral position and off-loading weight from ventilator circuit, are integral to maintaining skin integrity around a tracheostomy tube11,12. The exact mechanism and mechanical forces leading to skin injury caused by medical devices have not been fully explained23. Internationally recognised classifications for PI are widely accepted and new classification for mucosal injuries are now available1. However, an injury caused by a tracheostomy tube cannot be easily defined by either category.
An unexpected finding arising from this study was the lack of adherence and/or documentation of tracheostomy-related stoma cares by nursing staff. Given this was a retrospective audit, data recorded relies on what was documented in the patient’s chart; therefore, care may have been delivered but not recorded. The longest time cares not documented were for seven consecutive time-points (14 days), with this patient not developing a TRSI. A single patient was also found to not have documented cares for six consecutive time-points (12 days), as well as two patients with five time-points (10 days) and two patients with four time-points (8 days). None of these patients developed TRSI.
Previous work by Barakat-Johnson et al.2 supports this finding. Barakat-Johnson et al.2 identified that nursing staff have an awareness for the need of skin inspections for high risk patients; however, assessment of the skin underneath a medical device, i.e. the tracheostomy flange, was not something nurses identified they would do on a daily basis.
Limitations and strengths
To our knowledge this is the first study to review and describe TRSI in an adult ICU population which is not associated with models of care or tracheostomy care bundles. This study is limited by the sample size and sampling technique and there is likely an underestimate of the true incidence of PI development as many were not observed for the full 20-day period nor the full ICU length of stay. Therefore, we cannot be confident that this estimate is accurate.
Conclusion
This study addresses the tracheostomy tube, providing evidence regarding TRSI in the ICU setting, an area with limited research and data. Of the 102 patients who received a tracheostomy in the ICU, 23 (22.5%) developed a TRSI, indicating a high percentage of skin injury in this vulnerable patient population. In this study the use of non-adjustable flange tubes was associated with the development of TRSI; however, caution should be applied weighting this finding too heavily due to the small numbers of patients with adjustable flange tubes and the low proportion of patients who developed TRSI. Findings from this study also highlight a lack of adherence to procedure/guidelines and/or documentation by nursing staff in the provision of tracheostomy cares.
Acknowledgements
We thank Fiona Boch and Jessica Brown for their assistance with data retrieval.
Conflict of interest
The authors declare no conflicts of interest.
Funding
The authors received no funding for this study.
Author(s)
Karyn Heineger*
RN, Grad Cert (Wound Care)
Clinical Nurse Consultant Tracheostomy Management Service, Royal Brisbane and Women’s Hospital, QLD, Australia
Email karyn.heineger@health.qld.gov.au
Kathy Hocking
RN, Grad Dip (Wound Care)
Acting Clinical Nurse Consultant Skin Integrity Service, Royal Brisbane and Women’s Hospital QLD, Australia
Nanette Paxman
Physiotherapist – Advanced (Tracheostomy),
Royal Brisbane and Women’s Hospital,
QLD Australia
Stacey Llewellyn
BMaths BAppSc(Hons) MBiostatistics
Biostatistician, Statistics Unit, QIMR Berghofer
QLD Australia
Anita Pelecanos
BSc (Hons), BHSc (Hons)
Biostatistician, Statistics Unit, QIMR Berghofer
QLD Australia
Fiona Coyer
RN, MSc Nursing, PhD
Professor of Nursing, School of Nursing, Queensland University of Technology and Royal Brisbane and Women’s Hospital, QLD, Australia
Visiting Professor, Institute for Skin Integrity and Infection Prevention, University of Huddersfield UK
* Corresponding author
References
- European Pressure Ulcer Advisory Panel (EPUAP), National Pressure Injury Advisory Panel (NPIAP), Pan Pacific Pressure Injury Alliance (PPPIA). Prevention and treatment of pressure ulcers/injuries: clinical practice guidelines. The international guideline. 3rd ed. EPUAP, NPIAP, PPPIA; 2019.
- Barakat-Johnson M, Barnett C, Wand T, White K. Medical device-related pressure injuries: an exploratory descriptive study in an acute tertiary hospital in Australia. J Tissue Viability 2017;26:246–253.
- Barakat-Johnson M, Lai M, Wand T, Li M, White K, Coyer F. The incidence and prevalence of medical device-related pressure ulcers in intensive care: a systematic review. J Wound Care 2019;28(8):512–520.
- Cooper K. Evidence-based prevention of pressure ulcers in the intensive care unit. Critical Care Nurse 2016;33(6), 57–67.
- Hanonu S, Karadag A. A prospective, descriptive study to determine the rate and characteristics of and risk factors for the development of medical device-related pressure ulcers in intensive care units. Ostomy Wound Manage 2016;62(2):12–22.
- Delmore B, Ayello E. Pressure injuries caused by medical devices and other objects: a clinical update. Am J Nurs 2017;117(12):36–44.
- Gefen A, Alves P, Guido C, Coyer F, Milne C, Ohura N, Waters N, Worsley P. Device-related pressure ulcers: SECURE prevention. International consensus document. J Wound Care 2020;29(2):S1–51.
- Coyer F, Gardner A, Doubrovsky A, et al. Reducing pressure injuries in critically ill patients by using a patient skin integrity care bundle (INSPIRE). Am J Critical Care 2015;24(3):199–209.
- Mitchell R, Hussey H, Setzen G, et al. Clinical consensus statement: tracheostomy care. Otolaryngol – Head Neck Surg 2013;148(1):6–20. doi:10.1177/0194599812460376
- Bodenham A, Bell D, Bonner S, Branch F, Dawson D, Morgan P, McGrath B, Mackenzie S. Standards for the care of adult patients with a temporary tracheostomy. Standards & Guidelines, Intensive Care Soc Standards 2014.
- Morris L, Whitmer A. Tracheostomy care and complications in the intensive care unit. Crit Care Nurs 2013;33(5):18–31.
- Dixon L, Mascioli S, Gillin T, Upchurch C, Bradley K. Reducing tracheostomy-related pressure injuries. AACN Adv Criti Care 2018;29(4):426–431.
- Hess D, Altobelli N. Tracheostomy tubes. Respir Care 2014;59(6):956–970.
- O’Toole T, Jacobs N, Hondorp B, Crawford L, Boudreau L, Jeffe J, Stein B, LoSavio P. Prevention of tracheostomy-related hospital-acquired pressure ulcers. Otolaryngol – Head Neck Surg 2017;156(4):642–651.
- Coyer F, Stotts N, Blackman S. A prospective window into medical device-related pressure ulcers in intensive care. Int Wound J 2014;11(6):656–664.
- ANZICS Centre for Outcome and Resource Evaluation. 2018 Report. ISBN: 13:978-1-876980-55-9.
- Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med 1985;13(10):818–29.
- Putensen C, Theuerkauf N, Guenther U, Vargas M, Pelosi P. Percutaneous and surgical tracheostomy in critically ill adult patients: a meta-analysis. Crit Care 2014;18:544. doi:10.1186/s13054-014-0544-7
- Cooper K, McQueen K, Halm M, Flayter R. Prevention and treatment of device related hospital-acquired pressure injuries. Clinical Evid Rev 2020;29(2):150–154.
- Jackson D, Sarki A, Betteridge R, Brooke J. Medical device-related pressure ulcers: a systematic review and meta-analysis. Int J Nursing Stud 2019;92:109–120. doi:10.1016/j.ijnurstu.2019.02.006
- Sankovich K, Fennimore L, Hoffmann R, Ren D. The impact of education and feedback on accuracy of pressure injury staging and documentation by bedside nurses, Patient Safety, Sept 2019;10–17. doi:10.33940/HAPI/2019.9.2
- Haesler E. Evidence summary: pressure injuries: preventing medical device related pressure injuries. Wound Pract Res 2017;25(4):214–216.
- Black J, Kalowes P. Medical device-related pressure ulcers, Chronic Wound Care Manage Res 2016;6(3):91–99.

