
Ahead of Print
Demonstrating negative pressure wound therapy in the management of non-healing surgical wounds: a case series
Doreen Hölper, Rainer Schach, Joanne Handsaker, Catherine McCarthy
Keywords non-healing, evidence-based, holistic, NPWT, surgical wound
For referencing Hölper D, et al. Demonstrating negative pressure wound therapy in the management of non-healing surgical wounds: a case series. Journal of Wound Management. 2024;25(3):to be assigned.
DOI
10.35279/jowm2024.25.03.05
Submitted 19 March 2024
Accepted 20 June 2024
Abstract
Background Wounds continue to be of global concern, amid a lack of widespread adoption of evidence-based practice (EBP). Negative Pressure Wound Therapy (NPWT) is supported by a wealth of evidence and has been widely adopted to manage a broad range of wound indications. This case series demonstrates the safe and effective use of single use NPWT (sNPWT) in the management of non-healing surgical wounds, alongside optimised wound care strategies and interventions.
Aim To present how adopting sNPWT to manage non-healing surgical wounds, alongside a holistic approach to patient care can improve the clinical outcomes.
Management and outcomes Five case studies are presented from hospital and community healthcare settings. All patients had non-healing surgical wounds, and all received treatment with sNPWT; length of therapy days varied between 19 and 91 days. Following treatment with NPWT, three wounds healed, one reached near full approximation of wound edges, and one was managed palliatively with marked improvement in quality-of-life outcomes.
Conclusion In all five cases, the non-healing surgical wounds, either healed or improved substantially when treated with an evidence-based approach incorporating sNPWT alongside optimised wound care strategies and interventions.
Implications for clinical practice Holistic patient-centered care in conjunction with sNPWT may improve outcomes for patients experiencing non-healing surgical wounds.
Key messages
- In this case series we describe wound indications, treatment strategies and outcomes of five patients who presented with non-healing surgical wounds and received NPWT in conjunction with holistic assessment and individualised treatments plans.
- Our goal is to raise awareness of the benefits of bringing evidence-based practice into clinical wound management.
- Our results suggests that pro-active interventions that include holistic assessment and individualised treatment plans in conjunction with NPWT, are advantageous to treating non-healing surgical wounds.
Introduction
Wounds continue to be a global concern, often described as a silent epidemic and an under-reported public health issue, with significant health and economic impact. The alarming financial burden of wound care is widely discussed in the literature.1,2,3 It is estimated that 1–2% of the population in developed countries will experience a chronic or non-healing wound during their lifetime4 and approximately 2% of all hospitalised patients have a non-healing wound.5 This increase may be attributed to the global rise in prevalence of diabetes and obesity, as well as an ageing population; leading to large numbers of pressure ulcers (PUs), venous leg ulcers (VLUs), diabetic foot ulcers (DFUs) and open surgical/dehisced wounds.6 Across the literature chronic, hard-to-heal and non-healing wounds are terms which are used interchangeably but refer to the same wound category/definition. A non-healing wound is one that fails to heal with standard therapy in an orderly and timely manner and is independent of the wound type and etiology.7 In 2020, around 900,000 people in Germany were reported to suffer from non-healing wounds with the quality and effectiveness of their treatment, proposed to depend on the expertise of the treating physician.8 More specifically, the associated costs of surgical site complications, including open surgical wounds and/or dehiscence, to both the healthcare system and patients has been widely documented.9,10
In response to the rising burden of non-healing wounds; consensus panels, national forums, initiatives, and best practice guidelines have sought to address and alleviate issues that contribute to this global challenge.3,11,12,13,14-16 One suggested strategy to improve outcomes in non-healing wounds is the use of advanced treatment therapies, such as NPWT. Evidence suggests that NPWT, when used appropriately and integrated into existing care pathways, improves healing rates, reduces clinical time, prevents admission/re-admission and improves the patient experience.17 NPWT is one of the most effective and widely used interventions for challenging wounds.18 This therapy is used for a variety of wound indications,19 with an established and accepted mode of action.20 In open wounds, the mode of action of NPWT is to contract the wound edges reducing the wound size; to reduce wound volume; reduce oedema; stimulate angiogenesis and granulation tissue formation and improve tissue perfusion.21,22 Two systems of NPWT delivery exist and can be categorised by traditional NPWT (tNPWT) and single-use NPWT (sNPWT). The tNPWT is commonly utilised to manage large heavily exuding wounds and is delivered using an appropriate filler, either polyurethane (PU) foam or 0.2% Polyhexamethylene Biguanide (PHMB) specific gauze, shaped to the wound bed, and secured with a film drape to form a sealed system. The sNPWT is designed to manage low to moderate exuding wounds and involves the controlled application of sub-atmospheric pressure to a wound, using a sealed dressing connected to a vacuum pump.23 The development of sNPWT allows therapy to be used across multiple care settings with the additional benefit of a small, portable, easy to use and disposable device.24,17,25 Both modes of delivery of NPWT provide similar clinical benefits to a wound, but allow clinicians flexibility in terms of choice, based on wound and patient factors.25,18 Furthermore, a step-across approach of tNPWT to sNPWT (or vice versa) can be taken.
The following case reports demonstrate safe and effective use of tNPWT and sNPWT (using the RENASYS Touch and PICO 14 pumps, manufactured by Smith+Nephew, Hull, UK) as part of a planned treatment pathway in the management of non-healing, open surgical wounds. The treatment pathways included a variety of dressings until wound healing occurred or treatment objective was achieved, therefore it is important to clarify that NPWT was not used until full closure of the wounds. The term ‘surgical wound dehiscence/dehisced surgical wound’ (SWD) covers a wide scope of problems from small openings to total separation of the incision line following surgery. It is clinically defined as separation of previously closed margins of a surgical incision that has been made in the skin.21 SWD can occur at any time after surgery, but generally occurs 4–14 days after surgery.21 Therefore, for most patients, dehiscence happens after discharge, when the care of the patient is transferred to community teams to manage. Some wounds are left open to heal (if there is a risk of infection or if there has been significant tissue loss). These are known as ‘healing by secondary intention’. They are estimated to comprise approximately 28% of all surgical wounds and are frequently complex to manage.26 A dehisced/open surgical wound may or may not show signs of infection on assessment.
Table 1. Patient demographics and medical histories: An overview of each case, type and length of treatment with NPWT
Method
Aim
To demonstrate safe and effective use of both tNPWT and sNPWT as part of a routine treatment pathway in previously non-progressing dehisced surgical wounds when healing by secondary intention, in a real-world clinical setting.
Design
Five retrospective case studies were extracted from electronic patient medical records (EMR) by two German clinicians (General Practitioner and a Senior Physician in Surgery), between July 2020 and May 2021. All case reports were recorded on anonymised case templates. The clinicians were asked to complete case reports on patients where NPWT (either tNPWT and/or sNPWT) had been used as part of a treatment pathway for previously non-progressing wounds. Standard wound photography was used to record wound progression with patient consent for photographic images recorded in the EMR. Unfortunately, wound measurements or dimensions were not recorded within the EMR so are not included in this case report. The authors have followed the CARE guidelines for reporting for completeness in case reports.27
Participants
Patients with an open wound that had not progressed in an expected healing trajectory were included. There was no requirement to focus on a specific wound indication, however it is interesting that all the wounds captured were dehisced surgical wounds. Clinicians documented patient characteristics and wound care product utilisation until the wound had healed, or the treatment objective had been achieved.
Setting
Care and treatment decisions were made by the physicians, the patients were managed in a hospital clinic or home setting.
Case 1
Due to complications following coronary artery bypass surgery, the patient presented with an amputation wound. The wound was exhibiting clinical signs of infection and had been in a non-healing cycle for approximately one year. Initial treatment with sNPWT and an antimicrobial barrier dressing was initiated. Following 13 weeks of NPWT, the therapy was discontinued and stepped across to standard dressings, continued to healing (see Figure 1). The wound, present for approximately 52 weeks, achieved total closure at 25 weeks, following holistic assessment and an appropriate treatment plan. This enabled the fitting of a suitable prosthesis and substantial improvement to the patient’s quality of life.
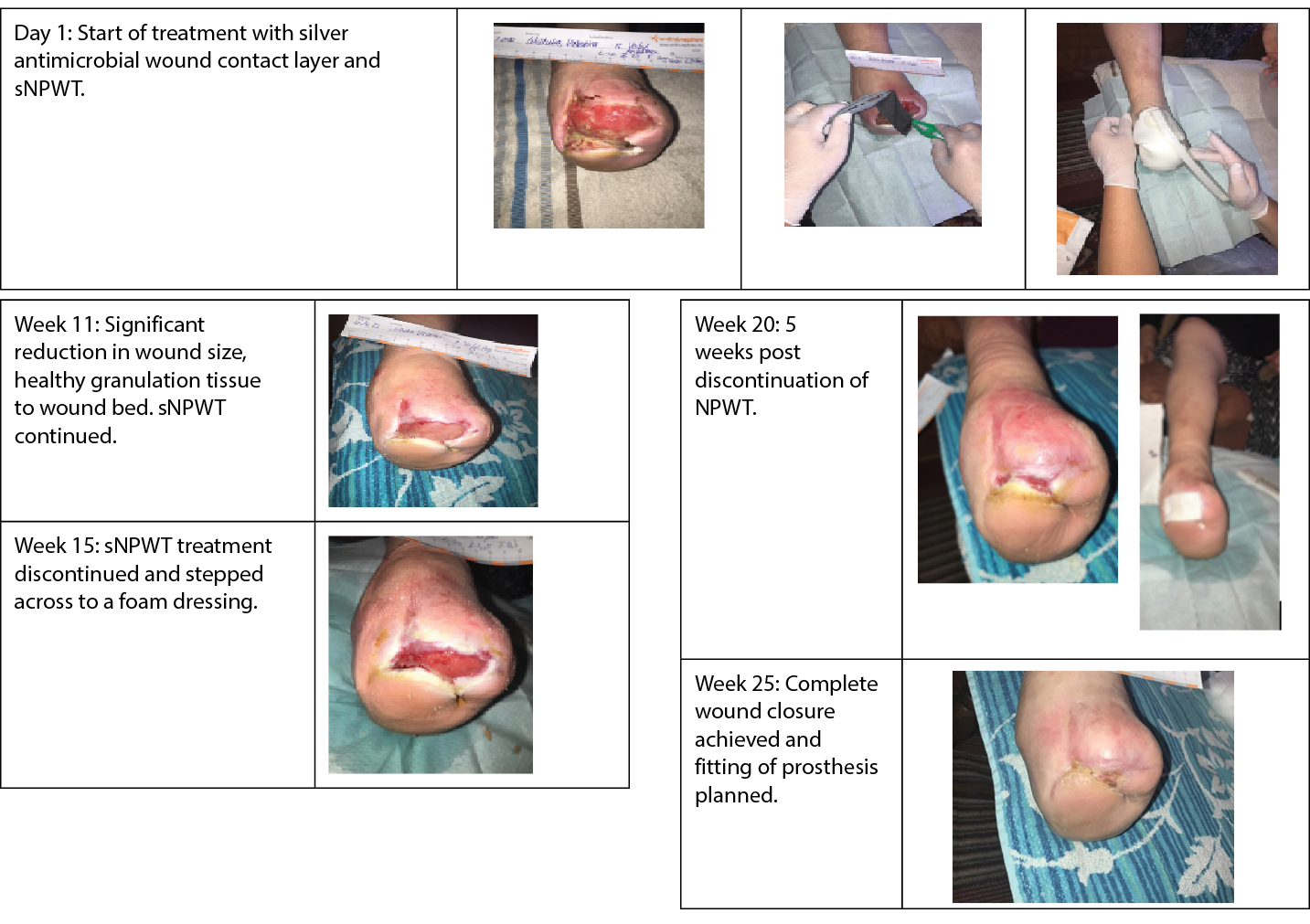
Figure 1. Case 1: Treatment and dressing application of a patient who experienced a forefoot amputation.
Case 2
Due to diabetic complications, the patient required a great toe amputation. The patient developed a wound infection and the wound dehisced, failing to respond to treatment with antimicrobial dressings. Following holistic assessment of the patient and wound, sNPWT in conjunction with an antimicrobial dressing was initiated. The antimicrobial dressing was stopped after two weeks and after nine weeks of NPWT the wound had reduced in size and sNPWT was discontinued. The wound was stepped across to standard wound dressings, continued to progress and total closure was achieved at 18 weeks (see Figure 2).
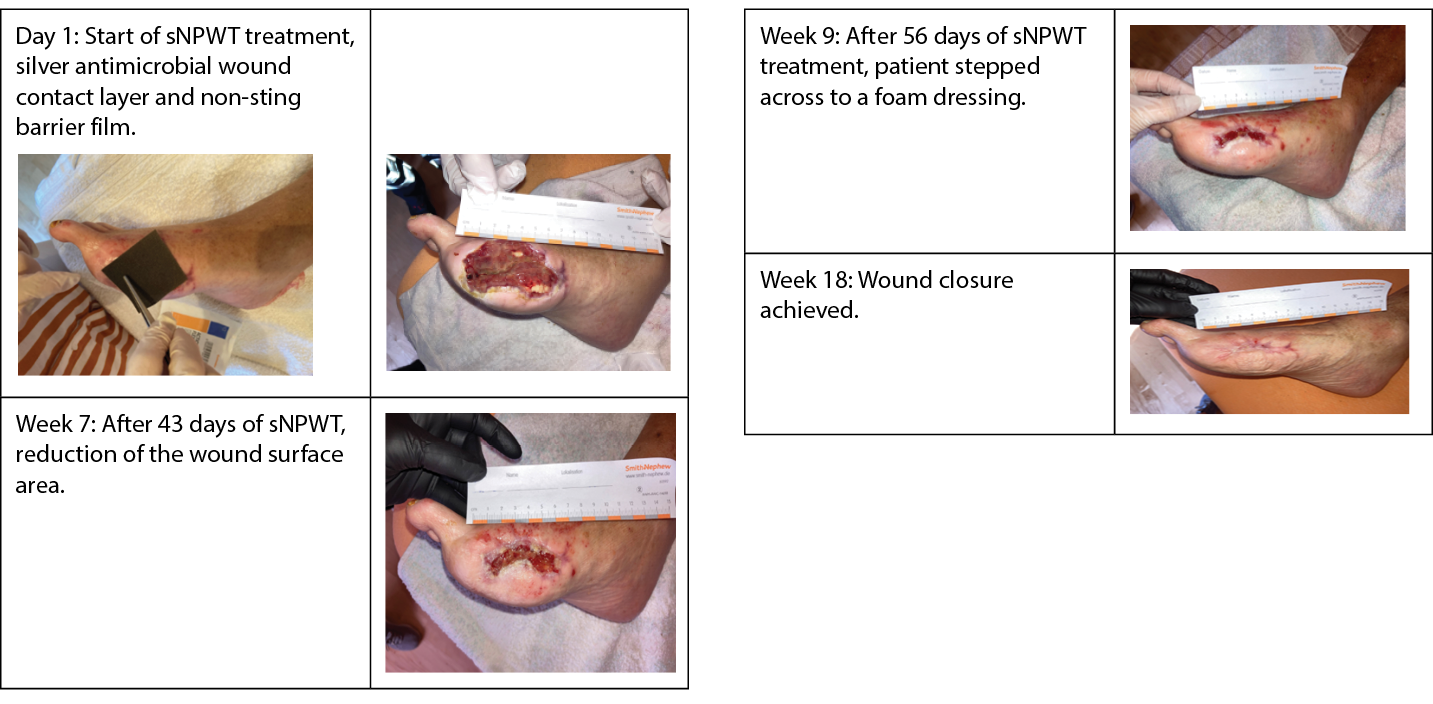
Figure 2. Case 2: Treatment and subsequent closure of an open wound post great toe amputation.
Case 3
The patient experienced a dehisced laparotomy incision following surgery for a peritoneal carcinomatosis induced colon perforation and faecal peritonitis. Post surgery the patient went into septic shock which forced a period of time. The proximity of the wound to the resulting, active ileostomy was a concern. tNPWT was initiated to manage the open wound reducing the risk of contaminants from the ileostomy. The wound progressed with tNPWT and was eventually stepped across to sNPWT at the point of discharge.
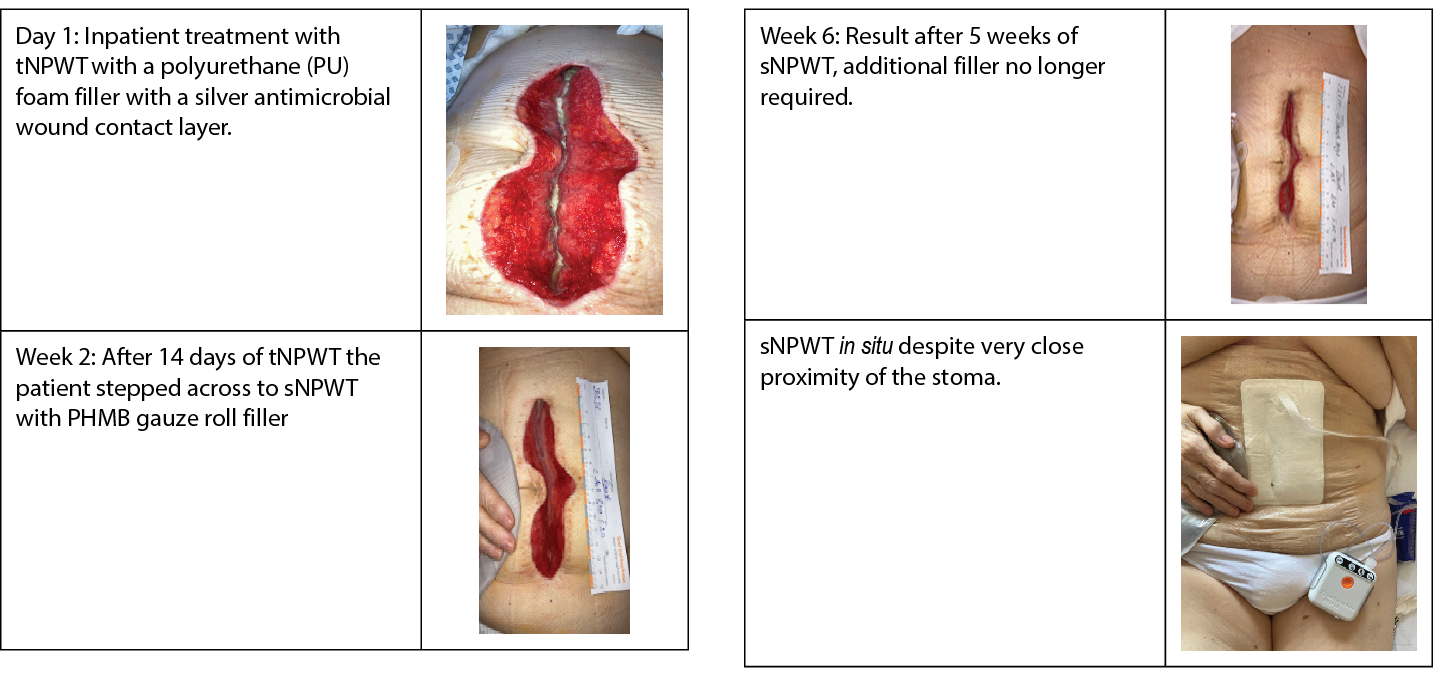
Figure 3. Case 3: A palliative case depicting successful management of complex abdominal wound near a stoma using sNPWT.
Case 4
The patient underwent emergency surgery following a perforated gastric ulcer, unfortunately the incision dehisced. tNPWT was commenced for five days and stepped across to sNPWT until closure (see Figure 4).
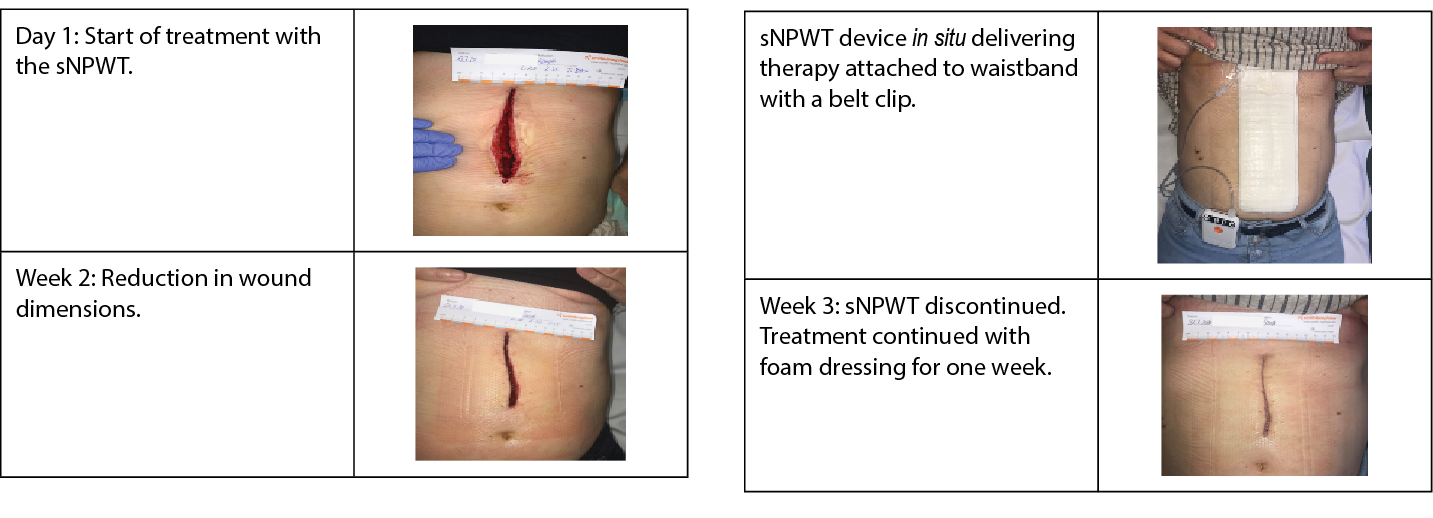
Figure 4. Case 4: Wound management through to closure of a dehisced laparotomy incision.
Case 5
The patient had an open ileocecal resection resulting in the formation of an ileostomy. The proximity of the wound to the stoma required careful consideration regarding treatment choice. tNPWT was initiated until the wound was appropriate to be stepped across to sNPWT. The patient was then managed with standard wound dressings at the point of near full approximation of edges, Figure 5.
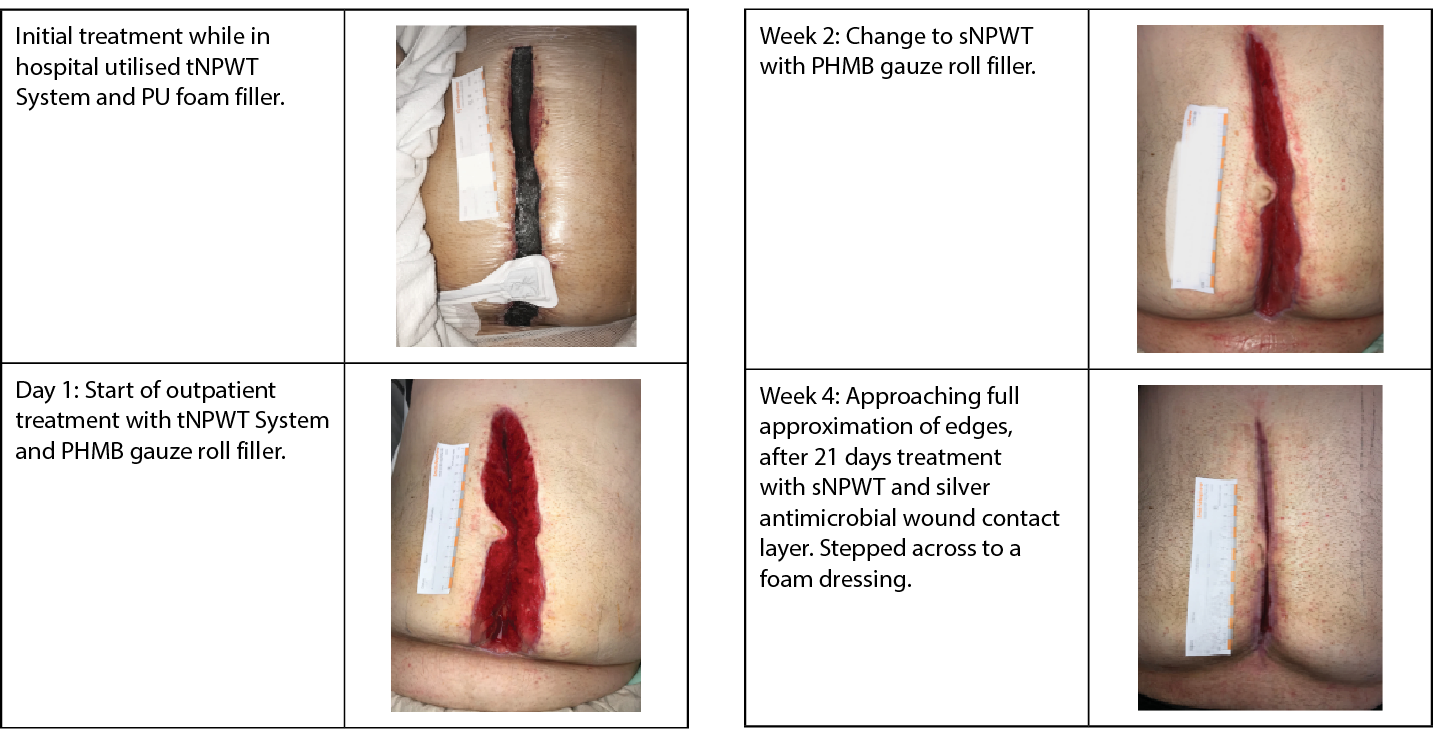
Figure 5. Case 5: Wound management of a dehisced laparotomy incision within an acute setting.
Discussion
Evidence-based practice (EBP) is advocated as vital to a patient’s chances of achieving successful healing outcomes3,28-31 and defined as the “conscientious integration of best research evidence with clinical expertise, patient values and needs in the delivery of high-quality, cost effective health care”.32 The ever-changing status of a non-healing wound bed means, that it is unlikely, one single dressing type and management approach can manage in totality the wound healing continuum.33 Careful assessment of the wound and the peri-wound tissues should inform dressing selection and dressing performance should be evaluated at each dressing change1.3,15,33,34 If wound improvement is noted, the current wound dressing regimen should be checked for suitability and adjusted if necessary.13
All the wounds presented were as a result of surgical intervention and in three cases wound dehiscence, following emergency colorectal surgery. This type of surgery carries higher risks compared to elective procedures due to the lack of preoperative preparation, risk of contamination and wound infection is a common cause of morbidity.35 SWD or wounds healing by secondary intention are a significant issue that affects large numbers of patients, their impact can be considerable including, increased mortality, delayed hospital discharge, readmission, further surgery, delayed adjuvant treatment, and impaired psychosocial wellbeing.16 All patients included in these reports had medical or surgical history that could potentially impact their wound healing trajectory and development of an infection. Open surgical wounds may become static or non-progressing, and alongside other wound indications, are becoming a socioeconomic emergency due to the high costs associated with hospitalisation that is required for wound management.
Strategies that can improve the management of these wound complications, include NPWT, and its benefits are widely reported in the literature.36 NPWT has a strong evidence base supporting its use and it is widely adopted for a broad range of wound indications.6,37 Though the application of NPWT is contraindicated for the treatment of malignant cutaneous wounds, as these lesions could granulate,38 there is still existing use and benefit to managing open wounds for a patient with a known cancer diagnosis.39 Despite this approach to care, the use of NPWT in these wound indications may still be considered as controversial. Many wounds in palliative care develop because of the effects of a non-curable, progressive disease that has weakened the healing process, preventing normal wound closure, despite treatment. It must be acknowledged that total wound healing and closure is sometimes unlikely, leading to the modification of wound management objectives, in conjunction with open communication with the patient, carers and other health care professionals.39,40 In scenarios where wound closure is unlikely, Chisholm (2010) suggests the focus of wound care should shift to agreed strategies to provide the patient with the most comfort in controlling symptoms, such as exudate management, frequency and comfort of dressing changes and reducing any negative impact on psychological or social wellbeing.39 A recent meta‐analysis assessing the risks and benefits of NPWT in surgical wounds with underlying malignant disease concluded that NPWT is not contraindicated in cancer surgical wounds and can be considered a beneficial palliative treatment to in managing open wounds.40,41 This approach was taken to support appropriate end of life care for the patient treated for peritoneal carcinomatosis. In this case, sNPWT provided successful and effective symptom control in terms of exudate management, reduction in dressing changes and increased quality of life for the patient.
The therapy has evolved beyond its original design as a stationary, reusable, traditional NPWT system, to offer the option of a single-use, portable device (sNPWT).42,43 The adoption of treatment strategies with established clinical efficacy, such as tNPWT and sNPWT, can improve the management of these wound complications. Patients can find the tNPWT pump and attachments difficult to move around with at home.25 This ‘step across’ approach is recommended by a consensus panel who support the transition between NPWT devices, based on wound dimensions, exudate levels, patient and care setting factors.44 Decision making on when to step across from one system to another can prove challenging to clinicians and the benefits of such require continuous demonstration and education. In response to this, an expert panel produced a clinical decision-making tree, supporting clinicians’ assessments when considering a move between available NPWT devices. The decision-making tree also provides clarity on when to step across to use a filler with sNPW, for example, for wounds over 2cm in depth a filler is advised.44 Widespread adoption of these recommendations has the potential to facilitate clinical decision making on which NPWT system is appropriate to use, to help optimise patient care and to minimise healthcare system expenditure.44 A step across from tNPWT to sNPWT approach was adopted in two reported cases, emphasising the benefits of product choice.
All patients included in these case reports accessed a range of wound care products that were deemed clinically appropriate to facilitate healing throughout the wound journey. Access to a range of products with a strong evidence base helped facilitate and standardise treatment selection, thereby increasing the likelihood of successful wound healing in most scenarios. It is important for healthcare practitioners to understand the key differences in the indications for use, precautions of various dressings and therapies. Selecting the clinically appropriate dressing or bandages can reduce healing duration, decrease bioburden and improve patients’ quality of life.6,34
Limitations
The authors acknowledge the addition of specific wound measurements alongside wound images would be beneficial to provide a robust overview of wound healing. It is also noted that this would be the standard format for reporting of cases. However, the documentation received from the clinicians collating the reports did not include this information.
Conclusion
NPWT has demonstrated effective results in open wounds28 and because of the versatility and innovation of a smaller lightweight system, the size and portability of sNPWT lends itself as an important choice, supporting patients’ independence and mobility. NPWT in conjunction with holistic assessment and individualised treatment plans, may be advantageous in the closure of surgical dehiscence and/or wounds that were intended to heal by secondary intention. This observational approach of presenting routine wound care offers real world examples of successful management of surgical wounds, that either healed or improved substantially. There is an urgent need for the adoption of advanced treatments, with established clinical efficacy, such as NPWT, that can improve the management of wound complications, while also assisting with successful wound healing.
Implications for clinical practice or future research
The current emergence and recognition of real-world evidence should be considered by all practitioners, and its value embraced. Routine data collection to enable creation of case reports that capture successful patient outcomes, should be encouraged. Therefore, enabling publication which builds on this valuable body of evidence that can be replicated across wound care settings to educate, demonstrate, and uphold best practice and utilisation of published evidence.
Implications for Clinical Practice
- Holistic patient centred care in conjunction with NPWT may improve outcomes for patients experiencing non-healing surgical wounds.
Future research
- Further research on other non-healing wound types would be beneficial to explore if the same improved outcomes are seen when utilising NPWT as part of wound management pathways.
Conflict of Interest
Miss J Handsaker and Miss C McCarthy are both employed by Smith and Nephew.
Funding
The authors received no funding for this study.
Author(s)
Doreen Hölper¹ MD, Rainer Schach² MD, Joanne Handsaker3, Catherine McCarthy4 BSc (Hons), PGDip, RGN, DN
¹Clinics Böblingen, Bunsenstrasse 120, 71032 Böblingen, Germany
²Facharzt für Allgemeinmedizin Hindenburgstr.53, 72160 Horb am Neckar, Germany
3,4Global Clinical Strategy Specialist, Global Clinical Strategy – Advanced Wound Management, Smith and Nephew, Watford,UK
*Corresponding author email catherine.mccarthy@smith-nephew.com