

Volume 40 Number 1
Investigating ICU nurses’ understanding of incontinence-associated dermatitis: an analysis of influencing factors
Liu Qiang, Lu Wan Xian, Pan Yan Bin and Shan Miao Hang
Keywords behaviour, ICU nurse; IAD; knowledge, attitude
For referencing Qiang L et al. Investigating ICU nurses’ understanding of incontinence-associated dermatitis: an analysis of influencing factors. WCET® Journal 2020;40(1):32-38
DOI https://doi.org/10.33235/wcet.40.1.32-38
Abstract
Objective To investigate the knowledge, attitude and behaviour of ICU nurses in relation to incontinence-associated dermatitis (IAD) in patients with urinary and bowel incontinence. Following this, to identify and analyse any influencing factors to provide a basis for the formulation of standard preventative procedures and preventative nursing strategies for IAD.
Methods Convenience sampling was used to survey ICU nurses’ knowledge, attitude and behaviour towards IAD. Between September and October 2019, a questionnaire designed by the researchers, that also gathered demographic data on the ICU nurses surveyed, was disseminated by the organisation’s information technology processes to 508 ICU nurses. Data were statistically analysed by SPSS22.0 software.
Results The total score obtainable within the questionnaire of staff knowledge, attitude and behaviour was (73.03±7.18). This score matrix was comprised of the following sub scores: knowledge (7.23±1.40), attitude (22.53±3.21), and behaviour (43.27±5.20). The working years of clinical nurses was the main factor influencing the knowledge, attitude and behaviour scores of ICU nurses’ understanding and management of IAD (p<0.05). Multiple linear regression analysis showed that the standard of the IAD prevention and incidence monitoring processes and daily management of IAD were correlating influencing factors of ICU nurses’ total IAD score (p<0.01).
Conclusion: ICU nurses’ knowledge of IAD improved. Similarly, ICU nurses’ attitudes towards IAD was better; however, there were differences between attitudes and practices of IAD. Managers in ICU should be more cognisant of the aetiology of IAD and ensure ICU nurses are educated in associated pathophysiology, risk factors, prevalence and incidence monitoring and root cause analysis of instances of IAD. Further, managers should promote the use of standard prevention and nursing management processes to reduce the incidence of IAD.
Introduction
Incontinence-associated dermatitis (IAD) is a common irritant contact dermatitis that occurs in patients with urinary or faecal incontinence, and may be exacerbated by mechanical factors such as trauma and friction. Clinically, IAD may present as erythematous skin that is pink or red, has poorly defined margins, or may show variable depths of skin loss with or without vesicles or bullae. The dermis may weep if exposed1.
The prevalence of IAD in international studies ranged from 5.7–22.8%, and the incidence ranged from 3.4–36.0%2,3. Domestic studies in China have shown that the prevalence of IAD in incontinent patients is 2.5–3.2%. Further, the incidence rate of incontinence in ICU patients is significantly higher than that in general departments4,5. Incontinence-associated dermatitis induces pain in patients, increases the risk of stress injury to affected skin from shear and friction, and can cause secondary infection. In addition, IAD increases the cost of treatment, increases nurses’ workload and presents nurses with significant clinical challenges6. Current global research on IAD has focused on the management and prevention of IAD7.
After assessing the risk for patients in developing IAD, it is particularly important to select the most effective interventions as well as following any standard organisational procedures. Therefore, this study aimed to investigate the status quo of the knowledge, attitude and behaviour of ICU nurses on IAD prevention, and to use the results of the study to provide a basis for formulating standard preventative and nursing care strategies.
Study objective
This study aimed to investigate the status quo of the knowledge, attitude and behaviour of ICU nurses on IAD prevention, and to use the results of the study to provide a clinical framework for formulating standard preventative and nursing care strategies for IAD.
Research methods
Convenience sampling was used to select the first 500 ICU nurses from our facility to participate in the study if they met study criteria and correctly filled out the study questionnaires. Inclusion criteria were stated as:
- Registered clinical nurses with more than 1 year’s work experience.
- Nurses who gave informed consent.
- Nurses who volunteered to participate.
Exclusion criteria included:
- Nursing experts involved in the design of the study questionnaire.
- Nurses currently undertaking further education, training or study.
- Nurses currently on maternity or private leave.
Research tools
General questionnaire
A general data questionnaire to capture study participants’ demographics was designed by the researchers. The fields included age, gender, level of hospital / clinical care, education, job title, years working, job levels and categories, ways of gaining knowledge about IAD, and any recent training time, as well as comprehension of the standard of the IAD prevention processes, IAD statistical rates and monitoring, and daily clinical care of IAD.
Knowledge, attitude and behaviour questionnaire
The questionnaire to examine ICU nurses’ knowledge, attitude and behaviour of IAD was designed by the researchers following an extensive literature research on questionnaire design. A small pilot questionnaire was evaluated for content validity by three wound/ostomy specialist nurses, three experts in skin assessment, management staff and other researchers with expertise small sample enquiry form questionnaires. The content validity index (CVI) of the questionnaire was 0.811, and the Cronbach’s coefficient was 0.843, showing good reliability and validity.
The final questionnaire consisted of three parts – knowledge, attitude and behaviour, with a total of 33 items.
The knowledge questionnaire contained 11 items, including the concept of IAD, risk factors, risk assessment, IAD grading, and the identification of clinical manifestations of pressure ulcers. For each item, ‘yes’ was 1 point, ‘no’ or ‘not sure’ was 0 point, and the total score ranged from 0–11 points. The higher the score, the better the knowledge of IAD.
The attitude questionnaire was used to ascertain the degree of ICU nurses’ understanding of standard nursing measures to be used by ICU nurses to prevent IAD. There were a total of seven items. A Likert 4 grading method was adopted to rate responses as: ‘strongly disagree’, counted as 1 point; ‘disagree’ as 2 points; ‘agree’ as 3 points; and ‘strongly agree’ as 4 points. The total score ranged from 7–28 points. The higher the score, the better the agreement on the importance of standard IAD prevention.
The behavioural questionnaire was used to understand concordance with implementation of standard nursing measures to prevent IAD in ICU nurses’ clinical practice. There were a total of 15 items. Similarly, a Likert 4 grading method was adopted, with 1 point for ‘never’, 2 points for ‘sometimes’, 3 points for ‘often’ and 4 points for ‘always’. The total score ranged from 15–60 points. The higher the score, the better the implementation of standard preventive IAD care measures.
Data collection methods
From September to October 2019, all questionnaires were uploaded to and data was collected through our facility’s internal information technology star platform. This ensured the quality of information collected and a process for invalidating questionnaires where the answer time was less than 120 seconds. In order to prevent duplication or multiple survey responses being received, only the first valid answer according to the IP address and answer time was accepted.
Statistical analysis
SPSS22.0 software was used for data entry and statistical analysis. Frequency, composition ratio, mean ± standard deviation were used to describe categorical data, one-way anova and t test were used to compare the differences of ICU nurses’ IAD knowledge, attitude and behaviour scores, and multiple linear regression was used to analyse the factors influencing ICU nurses’ IAD behaviour. Double-sided test, test level mean α=0.05. Statistically significant difference is measured at (p<0.005).
Results
General information
A total of 508 questionnaires were issued and 508 were recovered, of which 500 were valid, with an effective recovery rate of 98.4%.
Demographically, among the 500 ICU nurses, 7.8% were men and 92.2% were women. Participants’ ages ranged as follows: 33.2% were aged 20–25; 29.4% were aged 26–30, 29.8% were aged 31–40 and 7.6% were aged 40 and above. Years of clinical nursing service showed 9.2% had nursed for less than 1 year, 20.0% for 1–3 years, 41.4% for 4–10 years, 21.8% for 11–20 years, and 7.6% for more than 20 years. With regard to education, respondents had secondary technical school 7.6%, junior college 38.2%, and bachelor’s degree or above 54.2%. Professional titles included 36.4% as nurses, 38.6% as primary nurses, 21.2% as chief nurses, 3.8% as deputy chief nurses. Duties encompassed: responsibility nurse (71.8%), nursing group leader (16.2%), head nurse (8%), and wound stoma therapist (4%).
ICU nurses’ knowledge of IAD
ICU nurses scored 0–11 (7.23±1.40) points for their knowledge of IAD. The top three scoring items were ‘definition of IAD’, ‘location of IAD’ and ‘type of IAD skin protectant’, with the correct rates of 98.8%, 96.6% and 94.0% respectively. The next three highest scoring items were ‘local skin exposure to faecal fluid reduces PH and disrupts skin barrier function’, ‘use of skin humectant to protect faecal-impregnated skin in patients with IAD’, and ‘soft tissue skin lesions in patients with IAD from bottom to top’, with correct rates of 4.6%, 29.2% and 34.0% respectively.
ICU nurses’ attitude towards IAD
The score of ICU nurses on IAD was 7–28 (22.53±3.21). The three items with the lowest scores were ‘IAD quality control and monitoring should be carried out’, ‘early use of stool collection device when stool count exceeds 3 times or is not formed’, and ‘standard preventive procedures can reduce the incidence of IAD’. The scores were (2.61±0.84) points, (3.07±0.68) points, and (3.27±0.58) points respectively.
ICU nurses’ behaviour and IAD
ICU nurses scores in terms of behaviour and clinical understanding of the management of IAD ranged between 27–59 (43.27±5.20) points. The lowest scored three entries were ‘in the occurrence of IAD choose complex alum powder solution to clean local skin’, ‘for daily cleaning peri-anal skin in patients with IAD choose dry cleaning fluid’ and ‘using IAD risk assessment scale to evaluate the risk factors of patients’. The scores were (1.57±0.83) points, (1.85±0.66) points and (2.17±1.02) points respectively.
Univariate analysis of ICU nurses’ scores of IAD knowledge, attitude and behaviour
Univariate analysis showed that ICU nurses had different scores in IAD knowledge, attitude and behaviour based on their age and years of clinical nursing service. The post category of ICU nurses and the last time learning occurred to gain knowledge in IAD had different scores for IAD knowledge. ICU nurses with different gender, age, years of clinical nursing service, post level, hospital level, post category, professional title and education had different attitudes towards IAD.
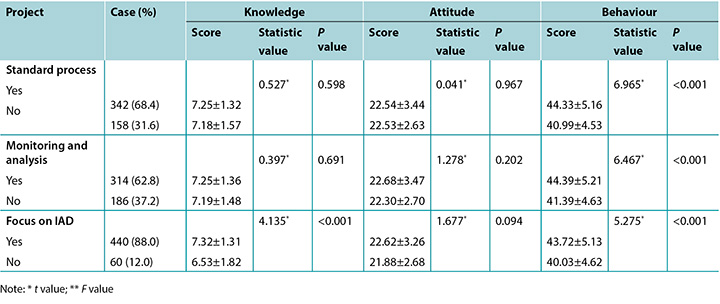
ICU nurses’ years of working as a clinical nurse, access to information on IAD knowledge, last time to gain knowledge of IAD, formulation of IAD standard prevention procedures, incidence monitoring and analysis of IAD, and daily attention to IAD, all had different scores for IAD. The difference was statistically significant (p<0.05). See Table 1 for details.
Table 1. Univariate analysis of knowledge attitude and behaviour of ICU nurses in preventing IAD (n=500, χ±Ѕ, points)
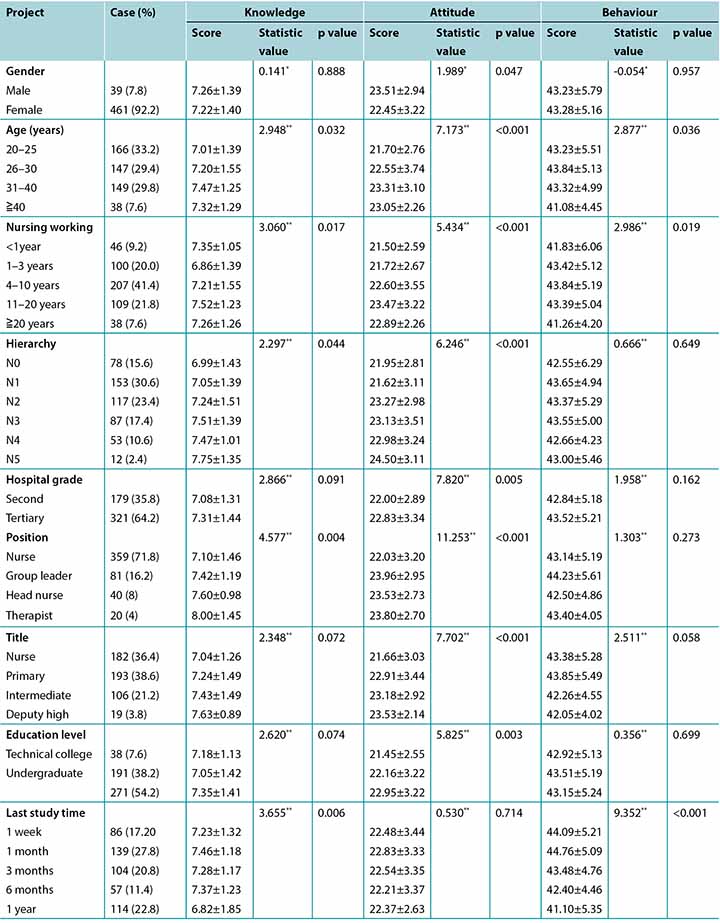
Table 1 continued. Univariate analysis of knowledge attitude and behaviour of ICU nurses in preventing IAD (n=500, χ±Ѕ, points)
Multivariate analysis of scores influencing ICU nurses’ IAD behaviour
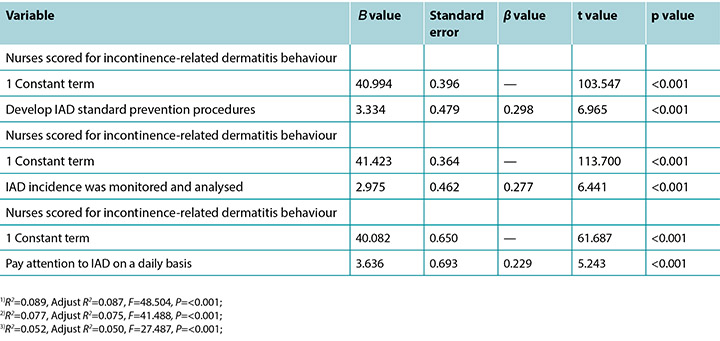
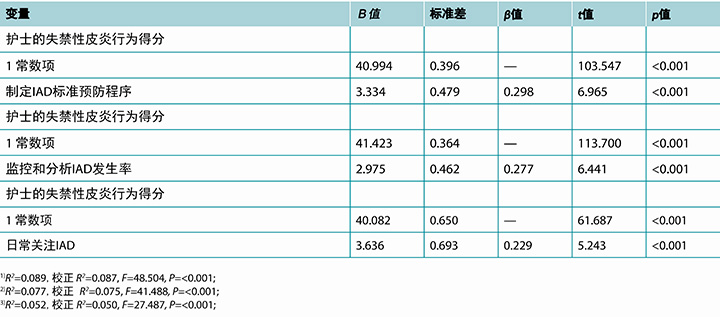
The score of ICU nurses‘ IAD behaviour was taken as the dependent variable, and the variables with statistical significance in the univariate analysis were taken as independent variables (assignment is shown in Table 2) for regression analysis (αenter=0.05, αeliminate=0.10). The results showed that the establishment of IAD standard prevention procedures, the monitoring and analysis of IAD incidence, and daily attention to IAD were the influencing factors of ICU nurses’ score of IAD (p<0.01) (see Table 3).
Table 2. Independent variable assignment
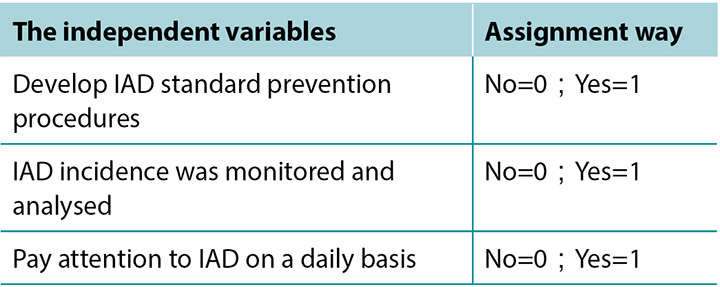
Table 3. Multi-factor analysis of IAD among ICU nurses
Discussion
The knowledge level of ICU nurses in preventing IAD needs to be improved
This study showed that the knowledge score of ICU nurses on the prevention and treatment of IAD was (7.23±1.40), from a total score of 11. ICU nurses who had been engaged in nursing work for 4–10 years had a higher knowledge of IAD (7.21±1.55), and the knowledge level of ICU nurses who had been engaged in nursing work for 1–3 years was lower (6.86±1.39); a statistically significant difference (p<0.005). These results show that ICU nurses’ knowledge of IAD is low and are similar to that reported by Xiao-xue Zhang8 who analysed the items ‘topical skin exposed to the fluid of the faeces’, ‘the Ph value decreased, destruction of skin barrier function’, ‘give IAD patients skin moisturiser to use to protect skin from faecal fluid’.
The results further suggest ICU nurses’ understanding of the pathogenesis of IAD, its resultant damage to the skin and secondary tissue stressors, and the correct selection of skin protectants to manage IAD is poor. In addition, there was a statistically significant difference in ICU nurses’ understanding of IAD-related knowledge among different job categories and the last time ICU nurses attended any education about IAD (p<0.05). This would suggest that managers should conduct systematic training for ICU nurses in the form of a flipped classroom model whereby staff are provide with information on IAD before participating in usual classroom style teaching to broaden understanding through discussion or other learning activities. This approach may also improve nursing staff’s participation in and interest in learning.
For nurses who have worked in clinical nursing for more than 20 years, ICU nurses of seniority and with senior positions had a good knowledge base and command of IAD, which may be related to their stricter role requirements, more internal and external learning opportunities, and accumulation of rich clinical experience9. The knowledge of IAD by wound stoma therapists is better than that of ICU nurses, which may be related to the systematic training of these specialist nurses which enhances their knowledge of IAD and associated disruption to skin integrity10. It is suggested that comprehensive basic nursing education and ongoing in-service education on IAD should be carried out, starting within undergraduate nursing programs.
ICU nurses’ attitude towards preventing IAD
The score for ICU nurses’ attitude towards IAD was (22.53±3.21) from a total 28 points. ICU nurses’ awareness of the pathophysiology, prevention and treatment of IAD was high, as can be seen from the results of the survey. Those ICU nurses with higher qualifications, higher clinical positions/titles and wound stoma therapists demonstrated a more positive attitude to understanding IAD and were more cognisant of the ramifications of IAD. Their personal and professional sense of responsibility and compliance with organisational procedures was also higher11.
In this survey, the item ‘conduct IAD quality control and monitoring’ was scored low. This may indicate the department may not have included the incidence of IAD in quality audit inspections, or the quality inspection results may be inconsistent with individual performance. The item ‘early use of stool collection device when stool count is more than 3 times or incomplete’ also had a low score, which may be because there were no stool collection sets available, or nurses lacked awareness of this protocol, or there was a lack of awareness of local skin risk assessment processes for incontinent patients in relevant departments. In regard to ‘standard prevention procedures can reduce the incidence of IAD’, the score was low, which may indicate insufficient attention may not have been paid by relevant departments to IAD prevention and treatment procedures, or that staff did not conform with departmental procedures. Therefore, it is particularly important to suggest the establishment of effective standard prevention and quality inspection procedures for IAD.
The behavioural level of ICU nurses in preventing IAD needs to be improved urgently
Evaluation of the results of this study showed that the total score of prevention behaviours of ICU nurses for IAD was 27–59 (43.27±5.20) points. Responses to the survey question, ‘the use of IAD risk assessment scale to evaluate the risk factors of patients with IAD’ was low. However, ICU nurses’ per shift behaviour scored higher in assessment of patients with skin conditions. This suggests the ICU nurses, when conducting daily skin assessments of incontinent patients, did not use the IAD risk assessment scale or the department did not provide a uniform standard IAD risk assessment scale. International studies suggest that all incontinent patients are at risk for IAD and, therefore, a personalised prevention plan should be implemented to reduce the risk of IAD and related stress injury to the skin’s IAD12.
In terms of skin cleansing methods for patients with IAD, the results of this study showed that ‘patients with IAD used compound alum powder solution to clean local skin’ had a low score, indicating that ICU nurses were not familiar with its pharmacological characteristics or had never been exposed to it. The low score for ‘daily cleaning of perianal skin in patients with IAD’ indicates that ICU nurses still use alcohol wipes or warm water with dry paper towels to clean perianal skin when removing faecal fluid from faecally incontinent patients. One study has reported that the use of a pH neutral soap with water may interfere with skin barrier function13. It is recommended that our facility uniformly use the ‘no-rinse’ skin cleaning fluid close to the pH value of the skin.
In relation to skin protection strategies for patients with IAD in this study, the question ‘ICU nurses use skin humectant to protect moist skin in incontinent patients’, scored low. This indicates that the lack of knowledge of skin protection measures for incontinent patients may lead to improper clinical behaviour in terms of prevention and treatment strategies. For patients with faecal incontinence, it is advisable to keep the skin dry by using protective skin agents after each cleaning14.
Factors influencing ICU nurses’ prevention of IAD
This study showed that ICU nurses of different ages and years of clinical nursing service had different scores on IAD knowledge, attitude and behaviour. ICU nurses of different genders, ages, years of clinical nursing service, post levels, hospital levels, post categories, professional titles and education had different scores on IAD. These outcomes are similar to the study of Guo Jin et al.15, but different from the study of Zhang Xiao Xue et al.16. The main reason for the differences between these study analyses may be that the distribution of different hierarchical structures in ICU nurses is quite different, which also reflects the actual structure and role of clinical nurses.
The access to IAD knowledge and the last time to receive education on IAD had different scores on IAD behaviour. It indicates that receiving recent education on IAD can change the focus and approach of ICU nurses and it also encourages them to learn the latest trends in the prevention and treatment of IAD at home and abroad by attending academic conferences and consulting the literature, thus further influencing their knowledge, attitude and behaviour towards ICU IAD. It is suggested that the training methods of nurses should be diversified to include modern media technology (e.g. online apps) which are easily accessible, and that the courses for IAD should be repeated regularly. These measures would make it easier for nurses to learn and improve their knowledge and skills of IAD.
Daily attention to IAD, formulation of IAD standard prevention procedures, monitoring of IAD incidence, and analysis of behaviours affecting ICU nurses’ IAD practices
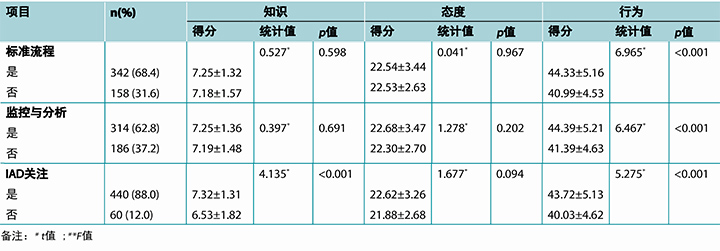
Study findings show that ICU nurses should pay closer attention to IAD in their daily practice and should develop and/or adhere to IAD standard prevention procedures. Meanwhile, monitoring and analysing the incidence of IAD are factors that influence ICU nurses’ IAD prevention behaviours. Currently, there are few relevant studies, especially those based on information-based monitoring of the incidence of IAD, to compare with. Na et al. studied and developed standardised nursing procedures for IAD which could reduce the risk of IAD in incontinent patients and improve the level of nurses’ knowledge of IAD prevention17. Jingru et al. used project management to prevent IAD in ICU patients, and the incidence of IAD decreased from 33.3% to 14%18. In the study, 68% of ICU nurses’ departments had developed IAD standard prevention procedures, indicating that IAD had attracted the attention of hospital managers, while 32% of ICU nurses’ departments did not develop IAD standard prevention procedures. The incidence of IAD was monitored and analysed in 62% of ICU nurses’ departments, while the incidence of IAD was not monitored and analysed in 38% of ICU nurses’ departments. While 88% of ICU nurses had daily clinical practice with IAD, 12% of ICU nurses had no daily IAD practice.
Study limitations
There are limitations in this study. First, on the basis of referring to a large amount of literature nationally and internationally, the researchers designed a questionnaire on IAD knowledge, attitude and behaviour of ICU nurses. Although the content validity and reliability of the questionnaire were tested, and the preliminary results showed the questionnaire had good reliability and validity, further tests are still needed. Secondly, the sample size of this study is still small and unevenly distributed, which may affect the accuracy of the results. Thirdly, more than 90% of participants in this study came from secondary and tertiary hospitals in Guangdong province, China, which did not cover all hospitals in this region; therefore, the convenience sample may not be reflective of all ICU nurses’ knowledge, attitude and behaviours of IAD. In the future, the authors need to revise and improve the questionnaire and carry out high-quality and large-sample data collection and research.
Summary
To sum up, the knowledge level of ICU nurses on the management and prevention of IAD still needs to be improved. There is a lack of systematic on-the-job IAD education and training. ICU nurses have a good attitude towards IAD prevention, with different attitudes and practical behaviours. Managers should promote and provide theoretical and clinical education on IAD and ensure clinical nurses know the pathophysiology, risk factors, and prevention and treatment strategies for IAD. Further, effective standard prevention procedures and preventive nursing strategies, so as to promote the standardisation of IAD nursing and reduce the incidence of IAD, should be developed.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
The authors received no funding for this study.
调查ICU护士对失禁性皮炎的理解:影响因素分析
Liu Qiang, Lu Wan Xian, Pan Yan Bin and Shan Miao Hang
DOI: https://doi.org/10.33235/wcet.40.1.32-38
摘要
目的 调查在大小便失禁患者中,ICU护士关于失禁性皮炎(IAD)的知识、态度和行为。此后,识别和分析影响因素,为制定IAD的标准预防程序和预防性护理策略提供依据。
方法 采用方便抽样法调查ICU护士对于IAD的知识、态度和行为。2019年9月到10月间,研究人员设计了一份调查问卷(包括收集受访ICU护士的人口统计学数据),并通过组织的信息技术流程分发给508名ICU护士。数据通过SPSS22.0软件进行统计分析。
结果 该医务人员知识、态度和行为调查问卷中,可获得总分为(73.03±7.18)分。该得分矩阵包括以下子项得分:知识(7.23±1.40)、态度(22.53±3.21)和行为(43.27±5.20)。临床护士的工作年限是影响ICU护士对IAD的理解和管理的知识、态度和行为得分的主要因素(p<0.05)。多元线性回归分析显示,标准IAD预防流程、IAD发生率监控和IAD日常管理是ICU护士IAD总分的相关性影响因素(p<0.01)。
结论 ICU护士对IAD知识有所改善。同样,ICU护士对IAD的态度变得更好;但是,IAD的态度和实践之间存在差异。ICU管理者应对IAD的病因有更明确的认知,确保ICU护士得到相关病理生理、危险因素、患病率和发生率监控及IAD病例根本原因分析等方面的教育。另外,管理者应提倡采用标准预防和护理管理流程,减少IAD发生率。
引言
失禁性皮炎(IAD)是一种常见的刺激性接触性皮炎,发生于大/小便失禁患者中,可能因外伤或摩擦等机械因素而恶化。临床上,IAD可能表现为粉红或红色皮肤红斑,边界不清,或者可能表现为不同深度的皮肤缺损,伴或不伴囊泡或大泡。如果发生接触,真皮可能渗液1。
国际研究发现,IAD患病率为5.7-22.8%,发生率为3.4-36.0%2,3。中国国内的研究发现,失禁患者的IAD患病率为2.5–3.2%。另外,ICU患者失禁发生率显著高于普通病房的患者4,5。失禁性皮炎引起患者疼痛,增加受累皮肤因剪切力和摩擦力而发生压力性损伤的危险,而且可能造成继发性感染。另外,IAD增加了治疗成本和护士的工作量,给护士带来重大的临床挑战6。目前世界上对IAD的研究重点在于IAD的管理和预防7。
评估患者患IAD的危险后,尤其重要的是,选择最有效的干预措施和遵守组织的所有标准程序。因此,本研究旨在调查ICU护士对IAD预防的知识、态度和行为现状,并利用本研究的结果提供制定标准预防和护理照护策略的依据。
研究目的
本研究旨在调查ICU护士对IAD预防的知识、态度和行为现状,并利用本研究的结果提供制定IAD标准预防和护理照护策略的临床框架。
研究方法
采用方便抽样法从我院选择第一批500名ICU护士,若符合研究标准且正确填写研究调查问卷,则参与本研究。入选标准如下:
- 注册临床护士,工作经验超过1年。
- 签署知情同意书。
- 自愿参与研究。
排除标准为:
- 参与设计本研究调查问卷的护理专家。
- 目前正在参与进修、培训或研究的护士。
- 目前休产假或事假的护士。
研究工具
一般情况调查问卷
研究人员设计了一般情况调查问卷来获得研究受访者的人口统计学数据。栏目包括年龄、性别、住院/临床护理水平、教育经历、职称、工作年限、工作级别和类别、获得IAD知识的方式、近期培训时间、对标准IAD预防流程、IAD统计率和监控及IAD日常临床护理的理解。
知识、态度和行为调查问卷
研究人员根据有关调查问卷设计的大量文献研究,设计了检查ICU护士在IAD方面的知识、态度和行为的调查问卷。先由3名伤口/造口专科护士、3名皮肤评估专家、管理人员和其他具有小样本调查表问卷专业知识的研究人员进行一次小型实验性调查问卷评估,以评估内容效度。本调查问卷的内容效度指数(CVI)为0.811,克朗巴哈系数为0.843,说明信度和效度良好。
最终调查问卷包括3个部分——知识、态度和行为,总计33个项目。
知识问卷含11个项目,包括IAD的概念、危险因素、危险评估、IAD分级、压疮临床表现的识别。对于每一个项目,“是”为1分,“否”或“不确定”为0分,总分范围为0–11分。得分越高,IAD方面的知识越好。
态度问卷用于确定ICU护士对用于预防IAD的标准护理措施的理解程度。共有7个项目。采用李克特4分量表将回答评分为:“完全不同意”计1分,“不同意”计2分,“同意”计3分,“完全同意”计4分。总分范围为7–28分。得分越高,说明对标准IAD预防措施重要性的认同度越高。
行为问卷用于了解ICU护士在临床实践中,采用标准护理措施预防IAD的一致性。共有15个项目。同样,采用李克特4分量表将回答评分为:“从不”计1分,“有时”计2分,“经常”计3分,“总是”计4分。总分范围为15-60分。得分越高,标准预防性IAD护理措施的实施越到位。
数据收集方法
2019年9月至10月,将所有调查问卷上传至本院内部信息技术星级平台并通过该平台收集数据。这确保了收集数据的质量,实施了当回答时间少于120秒时调查问卷无效的流程。为防止收到重复的2份或多份调查回复,根据IP地址和回答时间仅接受第1份有效回答。
统计分析
采用SPSS22.0软件进行数据录入和统计分析。采用频率、构成比、平均值±标准差描述分类数据,采用单因素方差分析、t检验来比较ICU的IAD知识、态度和行为的分的差异,采用多元线性回归分析影响ICU护士IAD行为的因素。双侧检验,检验水平为α=0.05。(p<0.005)表明差异具有统计学意义。
结果
一般信息
共发出508份调查问卷,收回508份调查问卷,其中500份有效,有效回收率为98.4%。
500名ICU护士的人口统计学特征为,男性7.8%,女性92.2%。受访者年龄范围如下:20-25岁占33.2%;26-30岁占29.4%;31-40岁占29.8%;40岁及以上占7.6%。临床护理工作年限为,9.2%的护理经验不足1年,20.0%为1-3年,41.4%为4-10年,21.8%为11-20年,7.6%超过20年。关于教育经历,7.6%的受访者为中等专科学校毕业,大专学历占38.2%,本科及本科以上学历占54.2%。职称为,护士占36.4%,初级护士占38.6%,护士长占21.2%,副护士长占3.8%。职务包括:责任护士(71.8%)、护理组长(16.2%)、护士长(8%)和伤口造口治疗师(4%)。
ICU护士的IAD知识
ICU护士的IAD知识得分为0–11分(7.23±1.40)。得分最高的前3项为“IAD的定义”、“IAD的部位”和“IAD皮肤保护剂类型”,正确率分别为98.8%、96.6%和94.0%。按得分高低顺序,较低的三个得分项目为“局部皮肤接触排泄液会降低PH值,破坏皮肤屏障功能”、“使用皮肤保护剂保护IAD患者皮肤不被排泄液浸渍”、和“IAD患者软组织皮肤病变为从下到上”,正确率分别为4.6%、29.2%和34.0%。
ICU护士对IAD的态度
ICU护士的IAD态度得分为7–28分(22.53±3.21)。得分最低的3个项目为“应执行IAD质控和监控”,“排便次数超过3次或大便不成型应尽早使用粪便收集装置”,和“标准预防程序可减少IAD发生率”。得分分别为(2.61±0.84)分、(3.07±0.68)分和(3.27±0.58)分。
ICU护士的IAD行为
ICU护士的IAD行为和对IAD管理的临床理解得分为27–59(43.27±5.20)分。得分最低的3个项目是“发生IAD时,选择合成明矾粉制剂清洁局部皮肤”、“日常清洁IAD患者肛周皮肤时选择干洗液”,和“使用IAD危险评估量表评估患者的危险因素”。得分分别为(1.57±0.83)分,(1.85±0.66)分和(2.17±1.02)分。
ICU护士的IAD知识、态度和行为得分的单变量分析
单变量分析显示不同年龄和临床护理工作年限的ICU护士,在IAD知识、态度和行为得分上存在差异。ICU护士的职务类别和最近一次学习IAD知识的时间对应的IAD知识得分不同。ICU护士的性别、年龄、临床护理工作年限、职务级别、医院等级、职务类别、职称和教育经历不同,对应的IAD态度也不同。
ICU护士作为临床护士的工作年限、对IAD知识的信息获取、最近一次学习IAD知识的时间、IAD标准预防程序的制定、IAD发生率监控和分析、IAD的日常关注,它们对应的IAD得分均有不同。差异具有统计学意义(p<0.05)。详情见表1。
表1. ICU护士在预防IAD方面的知识、态度和行为的单变量分析(n=500,χ ± Ѕ,分)
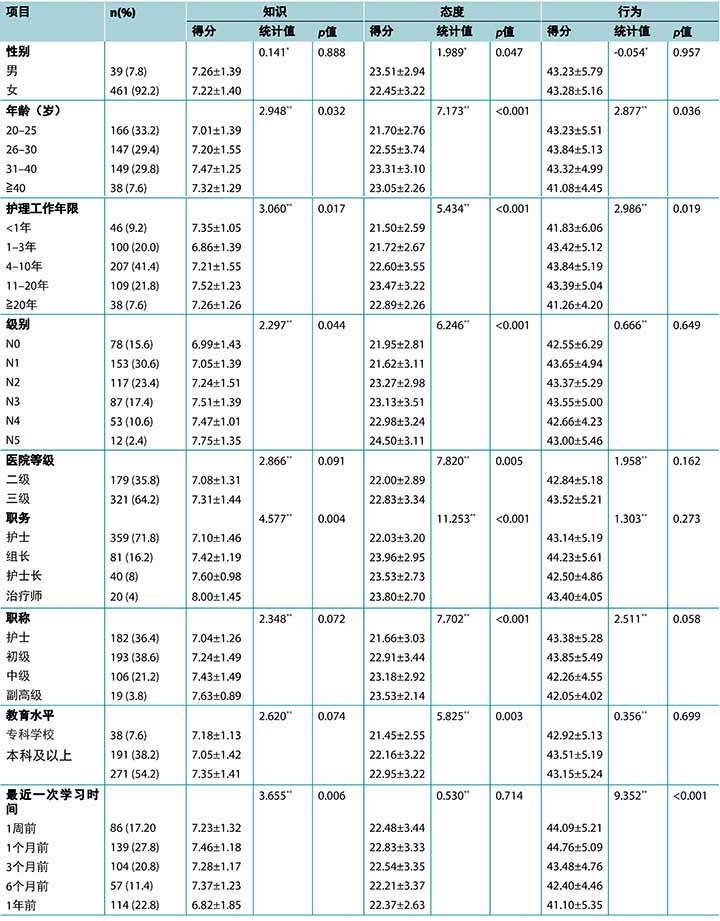
表1 续。ICU护士在预防IAD方面的知识、态度和行为的单变量分析(n=500,χ± Ѕ,分)
影响ICU护士IAD行为得分的多变量分析
在回归分析(α进入=0.05,α消除=0.10)中,将ICU护士的IAD行为得分作为因变量,将单变量分析中具有统计学意义的变量作为自变量(赋值见表2)。结果表明,制定IAD标准预防程序、IAD发生率监控和分析、IAD的日常关注是ICU护士IAD得分的影响因素(p<0.01)(见表3)。
表2. 自变量赋值
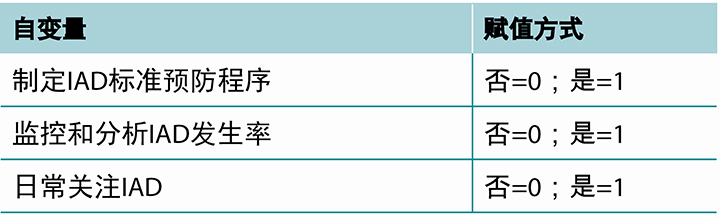
表3. ICU护士中的IAD多因素分析
讨论
ICU护士在预防IAD方面的知识水平尚需提高
本研究显示,ICU护士在IAD预防与治疗方面的知识得分为(7.23±1.40)分(总分11分)。从事护理工作4-10年的ICU护士具有更高的IAD知识得分(7.21±1.55),而从事护理工作1-3年的ICU护士知识得分较低(6.86±1.39);差异具有统计学意义(p<0.005)。这些结果表明,ICU护士的IAD知识水平较低,与Xiao-xue Zhang 8报告的结果类似,该研究分析了以下项目:“局部皮肤接触排泄液”、“Ph值下降,皮肤屏障破坏”、“给予IAD患者保护剂,保护皮肤不受排泄液损伤”。
本研究的结果还进一步表明,ICU护士对IAD病因及其导致的皮肤损伤、继发性组织压力源、以及正确选择皮肤保护剂管理IAD的知识很贫乏。另外,ICU护士的职务类别不同、最近一次参加IAD教育的时间不同,其对IAD相关知识的了解上也存在具有统计学意义的差异(p<0.05)。这表明,管理者应对ICU护士采取翻转课堂模式的方式进行系统性培训,借此在医务人员参加普通课堂模式教学之前先向他们提供IAD信息,通过讨论或其他学习活动拓宽他们的理解。这种方法还可提高护理人员的学习参与度和兴趣。
临床护理工作年限为20年以上的护士、资深ICU护士和高级职务ICU护士对IAD的知识水平和掌握程度较好,这可能与他们更严格的职责要求、内部外部学习机会更多、临床经验累积丰富有关9。伤口/造口治疗师的IAD知识水平好于ICU护士,原因可能是这类专科护士受过系统培训,强化了他们的IAD和有关皮肤完整性破坏的知识10。这表明,应展开全面的IAD基础护理教育和持续在职教育,从本科护理课程开始。
ICU护士对预防IAD的态度
ICU护士的IAD态度得分为(22.53±3.21)分(总分28分)。本调查结果表明,ICU护士对IAD病理生理、预防和治疗的了解程度较高。学历高、临床职务级别/职称高的ICU护士和伤口造口治疗师对理解IAD的态度更积极,对IAD分支的掌握程度更高。他们的个人责任感、职业责任感、对组织程序的遵从性更高11。
本调查中,“执行IAD质控和监控”一项的得分很低。这可能表明科室的质量审核检查中没有包括IAD发生率,或者质量检查结果可能与个人表现不一致。“排便次数超过3次或大便不成型应尽早使用粪便收集装置”一项得分也很低,可能是因为没有粪便收集装置可用,或护士缺乏对此方案的认识,或者相关科室缺乏针对失禁患者的局部皮肤危险评估流程的认识。还有“标准预防程序可减少IAD发生率”一项得分也很低,可能说明相关科室对IAD的预防和治疗程序没有给予足够重视,或者该医务人员没有遵守科室的程序。因此,特别重要的一点是,建议制定有效的IAD标准预防和质量检查程序。
亟需提高ICU护士在预防IAD方面的行为水平
对本研究的结果进行评估后显示,ICU护士的IAD预防行为总分仅为27–59分(43.27±5.20分)。调查问题“使用IAD危险评估量表评估IAD患者的危险因素”的回答得分很低。但是,在评估皮肤病患者时,ICU护士的每班行为得分较高。这说明ICU护士对失禁患者进行日常皮肤评估时没有采用IAD危险评估量表,或科室没有提供统一的标准IAD危险评估量表。国际研究表明,所有失禁患者都有患IAD的危险,因此,应实施个性化预防方案,减少IAD危险和皮肤IAD相关的压力性损伤危险12。
对于IAD患者的皮肤清洁方法,本研究结果显示,“对于IAD患者,采用合成明矾粉制剂清洁局部皮肤”一项的得分很低,说明ICU护士不熟悉该制剂的药理特性,或没有接触过该制剂。“对IAD患者肛周皮肤进行日常清洁”一项的得分很低,说明ICU护士在清除大便失禁患者排泄液时,依然采用酒精湿巾或温水加干纸巾清洁肛周皮肤。一项研究报告,使用中性pH值肥皂和水可能干扰皮肤屏障功能13。建议我院统一采用pH值与皮肤相近的“免冲洗”皮肤清洁液。
对于IAD患者的皮肤保护策略,本研究中,“ICU护士使用皮肤保护剂保护失禁患者皮肤不受潮湿”这一问题的得分也很低。这说明缺乏失禁患者皮肤保护措施的知识,在预防和治疗策略上可能导致不恰当的临床行为。对于大便失禁患者,建议每次清洁皮肤后使用皮肤保护剂保持皮肤干燥14。
影响ICU护士预防IAD的因素
本研究表明,不同年龄和临床护理工作年限的ICU护士在IAD知识、态度和行为上的得分也不同。ICU护士的性别、年龄、临床护理工作年限、职务级别、医院等级、职务类别、职称和教育经历不同,获得的IAD得分也不同。该结果也与Guo Jin等人15的研究结果类似,但与Zhang Xiao Xue等人16 的研究结果不同。上述研究分析存在差异的主要原因可能在于ICU护士的级别结构分布差异很大,这也反映了临床护士的实际结构和职责。
对IAD知识的获取,以及最近一次接受IAD教育的时间对应的IAD行为得分也存在差异。这说明近期接受IAD教育可能会改变ICU护士的关注点和护理方法,鼓励他们参加学术会议和查询文献,学习IAD预防和治疗方面的国内外最新趋势,从而进一步影响他们在ICU IAD方面的知识、态度和行为。建议对护士采用多元化培训方法,包括容易获取的现代媒体技术(如在线应用程序),还应定期重复举办IAD课程。这些措施将更便于护士学习并提高他们的IAD知识和技能
IAD的日常关注、IAD标准预防程序的制定、IAD发生率监控、ICU护士IAD实践的影响因素分析
研究结果表明,ICU护士应更多地在其日常实践中关注IAD,并应制定和/或遵守IAD标准预防程序。同时,IAD发生率的监控和分析也是ICU护士的IAD预防行为的影响因素。目前能够进行比较的相关研究很少,尤其是基于IAD发生率信息监控的研究。Na等人研究和制定了IAD标准化护理程序,可减少失禁患者的IAD危险,提高护士的IAD预防知识水平17。Jingru等人采用项目管理来预防ICU患者患上IAD,使IAD发生率从33.3%下降到14%18。本研究中,68%的ICU护士科室制定了IAD标准预防程序,说明IAD已经引起了医院管理层的注意,而32%的ICU护士科室没有制定IAD标准预防程序。有62%的ICU护士科室监控和分析了IAD发生率,而38%的ICU护士科室则没有。88%的ICU护士的日常临床实践中包含IAD,而12%的ICU护士则没有。
研究局限性
本研究存在若干局限性。首先,研究人员设计有关ICU护士的IAD知识、态度和行为的调查问卷时,参考了大量国内和国际文献。尽管调查问卷的内容效度和信度经过检验,初步结果也表明调查问卷的效度和信度良好,但尚需进一步检验。其次,本研究的样本量仍然较小并且分配不均,可能影响结果的准确性。再次,本研究超过90%的受访者来自中国广东省二级和三级医院,并没有覆盖该地区的所有医院;因此,方便抽样法可能无法反映所有ICU护士的IAD知识、态度和行为。未来作者还需要修订和改良调查问卷,进行高质量、大样本数据收集和研究。
总结
总之,ICU护士在IAD管理和预防方面的知识水平尚需提高。缺乏系统性在职IAD教育和培训。ICU护士对IAD预防的态度良好,但态度和实践行为之间存在差异。管理者应促进和提供IAD的理论和临床教育,确保临床护士了解IAD的病理生理、危险因素和防治策略。另外,应制定有效的标准预防程序和预防性护理策略,以促进IAD护理的标准化,减少IAD发生率。
利益冲突
作者声明无利益冲突。
资助
作者未因本研究收到任何资助。
Author(s)
Liu Qiang*
Undergraduate course, ICU nurse, the first affiliated hospital of Jinan University, Guangzhou city, Guangdong province, China
Email liuq469279208@163.com
Lu Wan Xian
Undergraduate course, head nurse, the first affiliated hospital of Jinan University
Pan Yan Bin
Master degree, ICU nurse, the first affiliated hospital of Jinan University
Shan Miao Hang
Undergraduate course, head nurse, the first affiliated hospital of Jinan University
* Corresponding author
References
- Beele H, Smet S, Van Damme N, Beeckman D. Incontinence-associated dermatitis: pathogenesis, contributing factors, prevention and management options. Drugs Aging 2018;35(1):1–10.
- Gates BP, Vess J, Long MA, Johnson E. Decreasing incontinence-associated dermatitis in the surgical intensive care unit: a quality improvement project. J Wound Ostomy Continence Nurs 2019;46(4):327–331.
- Gray M, Giuliano KK. Incontinence-associated dermatitis, characteristics and relationship to pressure injury: a multisite epidemiologic analysis. J Wound Ostomy Continence Nurs 2018;45(1):63–67.
- wen Z, Qixia J, Yanxia G, Yuhong Z. A multicentre study on the status and prevention of incontinence related dermatitis. J Med Graduate Students 2016;29(6):633–638.
- Suping T, Suibing R, Haishan X, Man L, Dongrong Z. Analysis of incontinence dermatitis in inpatients and its nursing measures. Chinese Nursing Ed 2015;12(7):554–557.
- Dorothy D, Joan J, Peter K, et al. Incontinence-associated dermatitis: consensus statements, evidence-based guidelines for prevention and treatment, and current challenges. Journal of WOCN 2012;39(3):303–315.
- Zhou Han YJ, hu Ailing ZL. Bibliometric analysis of nursing research on incontinence related dermatitis based on Web of Science. General Nursing 2019;17(11):1284–1287.
- Xiaoxue Z, Xinran W. Investigation on knowledge, practice, sources and needs of ICU nurses with incontinence dermatitis. Chinese Nursing Manage 2017;17(8):1119–1122.
- Yayan C, Duozi C. Investigation on the cognition status of incontinence dermatitis and structured nursing among 1429 nurses in bozhou. Anhui Medical 2019;40(5):573-577.
- Huan L, Ning N, Yongming T. Investigation on ICU nurses’ cognition of incontinence dermatitis in a hospital in Sichuan province. China J Practical Nurs 2013;29(27):64–66.
- Wanru X, Shiwei Y, Hui C, Lijuan H, Yajun P, Yi S. Investigation of 46 skin management liaison staff on prevention of incontinence related dermatitis. J Nurs 2017;24(4):51–55.
- Nelson K. The prevention and treatment of incontinence-associated dermatitis. Br J Nurs 2018;27(19):1101–1102.
- Beeckman D, Verhaeghe S, Defloor T, Schoonhoven L, Vanderwee K. A 3-in-1 perineal care washcloth impregnated with dimethicone 3% versus water and pH neutral soap to prevent and treat incontinence-associated dermatitis: a randomized, controlled clinical trial. J Wound Ostomy Continence Nurs 2011;38(6):627–634.
- Qiaoyan L, Meifen S, Chao W, Zhuo W, Jianping D, Zunjia W. Investigation and analysis of incontinence and incontinence related dermatitis. China J Practical Nurs 2015;31(33):2545–2549.
- Jing G, Huiping Y, Lifang Z, et al. Investigation on the status of knowledge and practice of incontinence dermatitis among ICU nurses in island area and analysis of influencing factors. Chinese Study Maternal Child Health 2017; 28(S3):530–531.
- Xiaoxue Z, Xinran W. Investigation on knowledge, practice and knowledge demand of incontinence dermatitis of ICU nurses in grade a hospitals in Beijing. Nurs Res 2017;31(33):4257–4259.
- Na L, Yanjun L, Lei G. Analysis on the effect of standardized nursing process on prevention of incontinence related dermatitis in elderly patients with incontinence. J Practical Clin Med 2019;23(16):114–120.
- Jingru L, Wanxian L, Qiang L. The effect of project management on prevention of incontinence related dermatitis in ICU patients. J Nurse Develop 2017;32(6) 550–552.
