
Volume 44 Number 1
Treatment of chronic parastomal ulceration with silver sulfadiazine and hyaluronic acid: a case series
Alison Carlin
Keywords wound, peristomal skin, hyaluronic acid, silver sulfadiazine
For referencing Carlin A. Treatment of chronic parastomal ulceration with silver sulfadiazine and hyaluronic acid: a case series. WCET® Journal 2024;44(1):36-39.
DOI
10.33235/wcet.44.1.36-39
Submitted 14 September 2023
Accepted 27 November
Abstract
Skin complications in ostomates are widely reported and can cause physical and emotional challenges in everyday life. Chronic parastomal skin complications can be difficult to heal and cause significant pain.
Two patients presented to the stomal therapy clinic for treatment and were diagnosed with chronic parastomal skin ulceration. Following standard treatment of wound management, topical corticosteroid ointment and appliance review, the ulcers were either not improving or had reoccurred. Treatment with a combination cream consisting of 0.2% Hyaluronic acid (HA) and 1% Silver sulfadiazine (SSD) was initiated and both patients demonstrated complete healing.
Treatment of parastomal skin ulceration with dual action cream 0.2% HA and 1% SSD was successful for these two patients, with a reduction in pain and purulent fluid noted throughout treatment, in addition to a reduced cost of treatment when compared with standard protocols.
Introduction
The risk of an ostomate developing a peristomal skin complication in their lifetime has been estimated as anywhere from 6–80%1. Ostomates with a skin complication report negative body image at a greater rate2. Male ostomates with a skin complication were 1.72 times more likely to report negative body image than ostomates with no skin complications, and female ostomates were even higher at 1.87 times more likely to report negative body image2. These complications account for approximately 40% of all visits to stoma care nurses3.
Peristomal and parastomal skin complication causes can be complex and include chemical injury, skin trauma, infection, contact dermatitis and disease related conditions4. Peristomal skin complications are more common in patients with an ileostomy (57%) and a urostomy (48%) than those with a colostomy (35%)5. Although peristomal skin complications, including ulcers, are quite common, chronic parastomal ulcers are unusual and can be difficult to manage6.
Ostomates who develop parastomal ulcers often have underlying conditions such as Crohn’s disease, irritable bowel disease (IBD) or Pyoderma gangrenosum (PG). Treatment and management of a parastomal ulcer consists of appliance review, wound care, systemic treatment (if patient has Crohn’s disease, IBD or PG) and local treatment, usually a corticosteroid6. If a patient does not have Crohn’s disease, IBD or PG, their parastomal ulcer is likely to respond quickly to local wound treatment6. Symptoms often include pain, appliance difficulties and leakage6. Often these ulcers may not look severe, but ostomates describe a strong burning pain, exacerbated by appliance changes6.
Stoma-associated skin complications have a wide ranging impact on an ostomate’s quality of life, and it is vital they are resolved quickly. The aim of this case study is to examine two ostomates with parastomal ulceration in which the standard treatment plan failed, with ostomates then trialling a new combination treatment of 0.2% Hyaluronic acid (HA) and 1% Silver sulfadiazine (SSD).
Product action
HA induces an accelerated tissue repair reaction, characterised by the growth of well-organised granulation tissue. HA receptor binding engages endothelial cells, macrophages, fibroblasts and keratinocytes and modifies their properties toward a more “repair oriented” condition7,8. In addition to stimulating cellular repair mechanisms, the substantial water binding capacity of HA molecules provides ideal conditions for migration and reproduction of the cells that form new tissue7,8.
SSD is a combination of two antimicrobial agents (silver and sulfadiazine) with broad spectrum antibacterial properties and is especially effective against those micro-organisms often found in infected skin lesions9. Applied on exudative wounds, SSD releases its silver ions, which increase the bacteriostatic effect of the sulfonamide radical. The sustained antimicrobial action of the sulfadiazine and silver combination is due partly to the continuous interaction with the fluids on the wound bed, which induces a slow, prolonged release of silver9.
Combination treatment of HA plus SSD (HA+SSD), as compared to SSD alone, has been proven to accelerate the repair process while also providing broad spectrum antibacterial action10. Clinical studies have demonstrated using the combination product of HA+SSD resulted in a reduction of nursing time, expenses and use of pain relief medication11,12.
Case presentations
Case 1
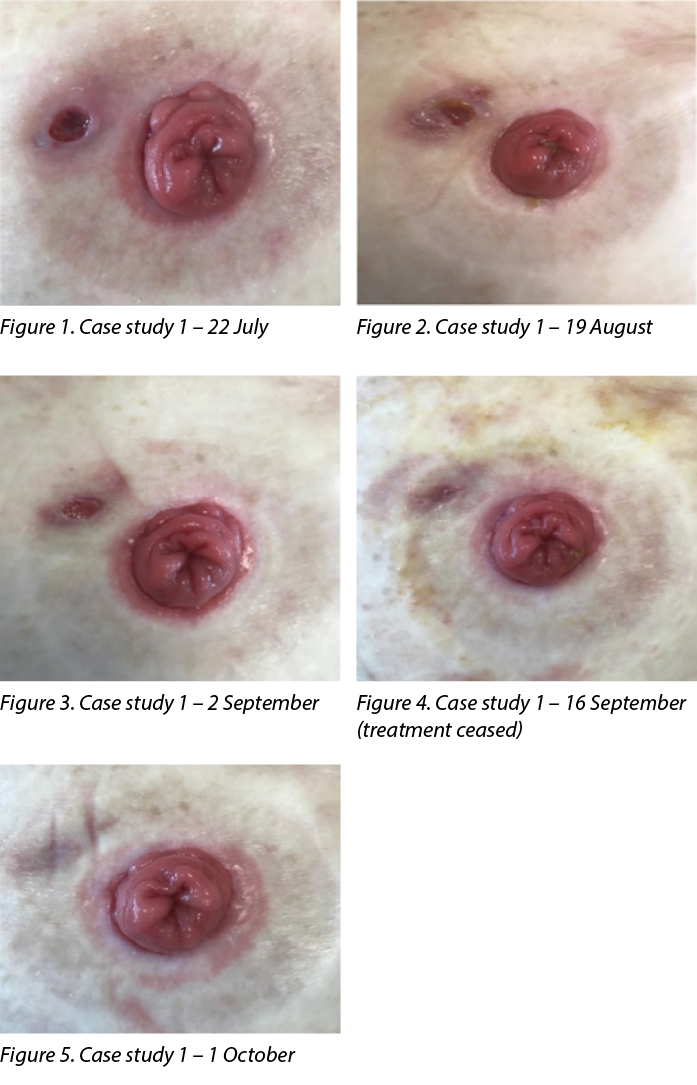
Patient TW is an 80-year-old female who underwent a total proctocolectomy with formation of an end ileostomy in May 2020. The patient’s ileostomy was healthy and the peristomal skin remained intact until she presented to the stomal therapy outpatient clinic in July 2021 with an ulcer of unknown aetiology. The ulcer measured 80mm x 50mm and was adjacent to her stoma at 10 o’clock. There was no pain and no odour noted, with low serous exudate and a soft base of the wound.
Management and outcome
Treatment initiated on 22 July 2021 (Figure 1) was a corticosteroid ointment, a silver antibacterial barrier dressing and a hydrocolloid dressing. The dressing was changed daily in conjunction with changing their ostomy appliance. After 1 month of treatment (Figure 2) the wound was 100mm x 50mm, with a clean base and purulent fluid present. The peri-wound skin was fragile and at risk of further breakdown. The patient’s colorectal surgeon had considered a biopsy to rule out infection of the wound with PG if the wound continued to show no signs of improvement.
The initial treatment was ceased and treatment with a cream containing 0.2% HA and 1% SSD was initiated (HA+SSD). Treatment was daily in conjunction with changing their ostomy appliance, which was the patient’s preference (Figure 3).
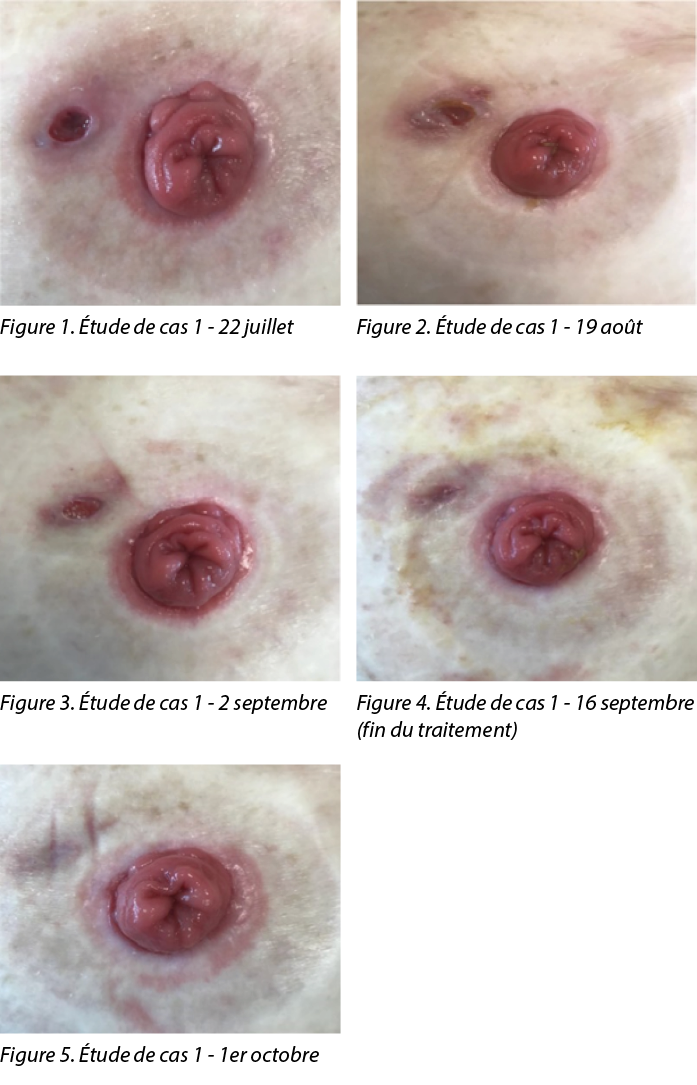
Following treatment with HA+SSD cream the wound continually reduced in size until it was healed. There was no pain or odour noted and the serous exudate reduced. On 16 September (Figure 4) treatment was ceased and the patient was advised to restart treatment if any break down of the wound reoccurred; however, the wound continued healing (Figure 5) and has remained healed almost 12 months later.
The treatment cost of standard vs combination HA+SSD treatment showed significant differences (Figure 6). The combination SSD + HA treatment was greater than 40% less expensive per dressing change, with only 25% of the tube being used in total.
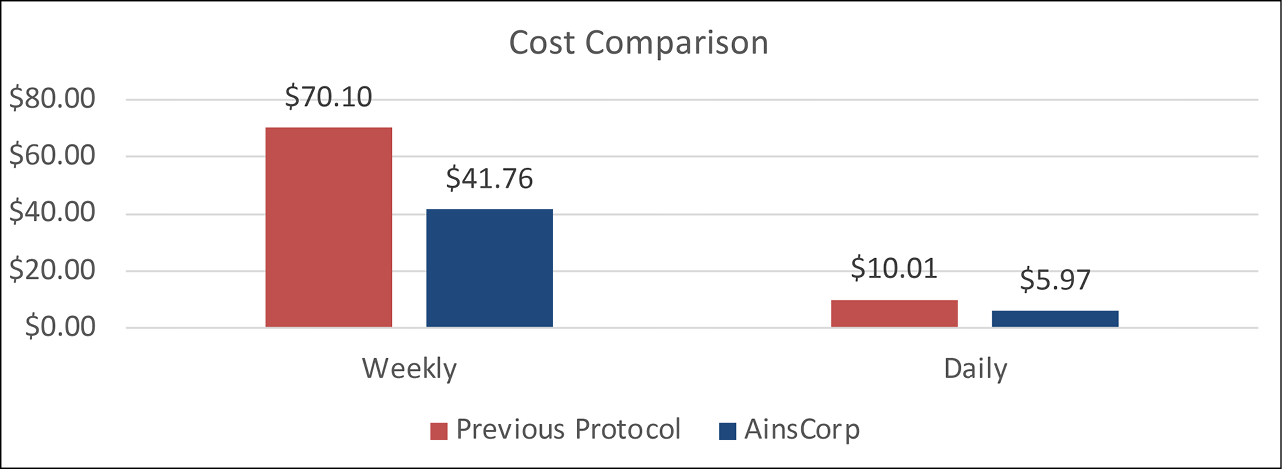
Figure 6. Case 1 – cost comparison of standard treatment vs combination HA+SSD treatment on a weekly and daily basis
Case 2
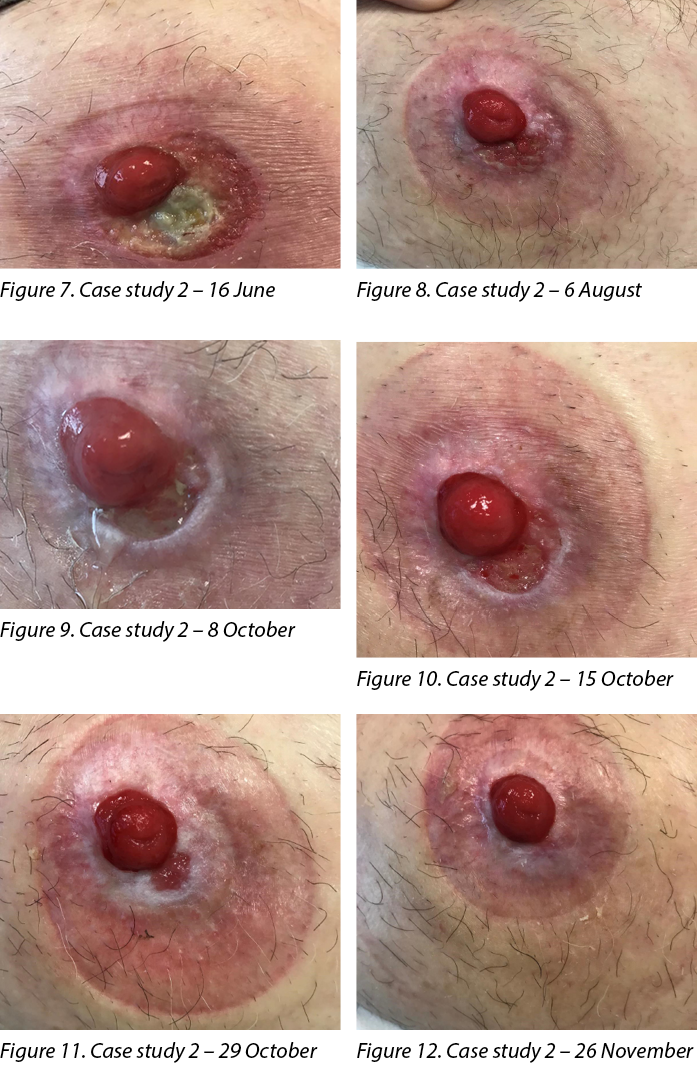
Patient ML is an 84-year-old male who had an ileal conduit formed in 2007. The patient’s ileal conduit and peristomal skin was healthy following surgery and had not been reviewed by a stomal therapist in 11 years. The patient presented to the stomal therapy outpatient clinic in June 2021 with peristomal ulceration and skin loss. The ulcer measured 20mm x 40mm and extended from the stoma edge from 12 o’clock to 7 o’clock. The ulcer was extremely painful with a sloughy base, low serous exudate and no oedema or odour.
Management and outcome
Treatment initiated on 16 June 2021 (Figure 7) was a corticosteroid ointment every second week, a silver antibacterial barrier dressing and a large and a small hydrocolloid ostomy seal. The dressing was changed according to patient preference and when the ostomy appliance leaked, which ranged from once per day to once per week.
Following 6 weeks of treatment (Figure 8), the ulcer was healed and treatment was ceased; however, the new granulation tissue in the 5 o’clock to 7 o’clock section of the ulcer appeared to be very fragile. The patient then re-presented on 8 October with the ulcer having broken down again (Figure 9). The wound measured 10mm x 5mm, with a sloughy pale base, wound edge maceration, low exudate and no pain, no oedema and no odour. At this stage the patient reverted to the initial treatment regime of a corticosteroid ointment every second week, a silver antibacterial barrier dressing and a hydrocolloid ostomy seal. The dressing was changed every 2–3 days, in conjunction with the ostomy appliance.
After 1 week (Figure 10) the wound was increasing (10mm x 20mm) and the initial treatment was ceased and treatment with a cream containing 0.2% HA and 1% SSD was initiated (HA+SSD). Treatment ocurred every two days in conjunction with changing their ostomy appliance, which was according to patient preference.
Following treatment with HA+SSD cream the wound continually reduced in size until it was healed. Two weeks following initial treatment (Figure 11) the wound had reduced from 10mm x 20mm to 5mm x 5mm. There was pink granulation tissue, low serous exudate and some maceration noted at the wound edges. No pain, oedema or odour were noted. Six weeks following treatment (Figure 12) the wound had healed and has since remained healed.
The treatment cost of standard vs combination HA+SSD treatment showed significant differences (Figure 13). The combination HA+SSD treatment was greater than 50% less per dressing change, with only 25% of the tube being used in total.
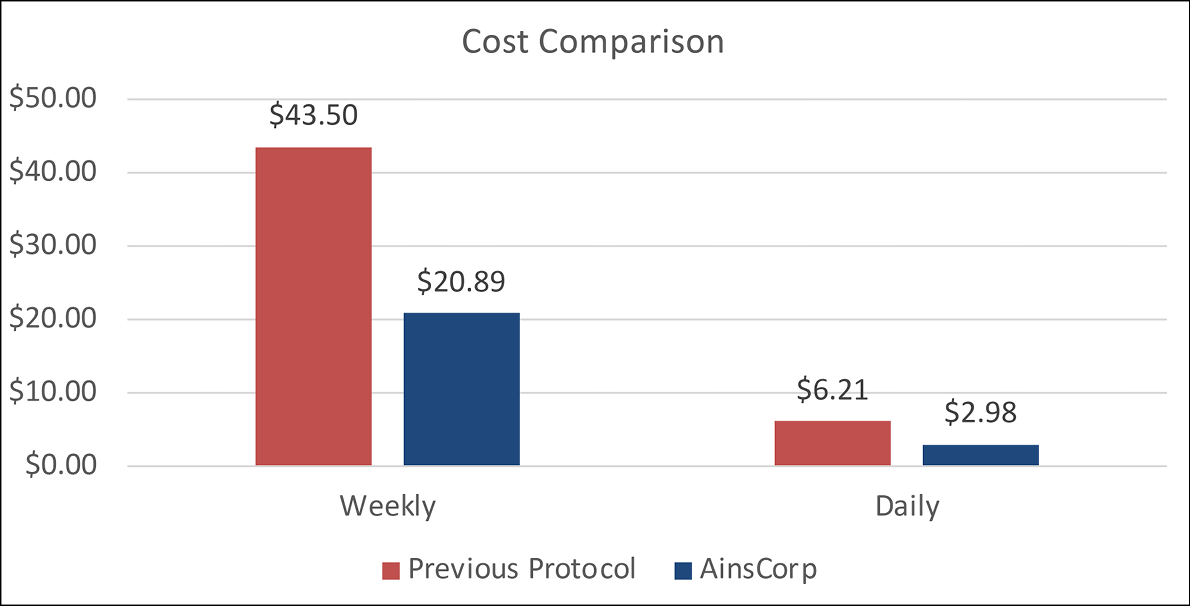
Figure 13. Case 2 – cost comparison of standard treatment vs combination HA+SSD treatment on a weekly and daily basis
Discussion
Both patients presented with parastomal ulcers of unknown aetiology which did not resolve with standard treatment. Following treatment with combination cream treatment 0.2% HA and 1% SSD (HA+SSD) the ulcers were successfully managed and healed. A small pea-sized amount of the combination cream was applied in a thin layer directly to the ulcer using a Q-tip, with no secondary dressing and the ostomy appliance applied on top. The application of cream underneath the baseplate did not affect adhesion of the hydrocolloid, and both patients reported no leakage or baseplate lifting prior to their pouch change schedule. This treatment facilitated discharge of patients from stomal therapy clinic, and both ulcers have remained healed since.
Conclusion
The cost of standard treatment compared to combination treatment of HA+SSD was significant. For Case 1 the cost of standard treatment was 1.68 times higher than the combination treatment, and for Case 2 the cost of standard treatment was 2.08 times higher than the combination treatment. In addition, the standard treatment failed for both patients and the wounds were still not healed after weeks of treatment, whereas the cost of combination treatment was calculated as time to wound healing. The significant cost difference of the HA+SSD combination cream compared to standard parastomal ulcer treatment (not taking into account additional GP reviews for scripts of Kenacomb®) indicates it could be an effective, low-cost intervention which could be applied at first presentation of a parastomal ulcer.
Acknowledgements
The patients consented to the use of their information for this case study. Photographs were taken with the patients’ verbal and written consent.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
The authors received no funding for this study.
Traitement de l'ulcération parastomiale chronique par la sulfadiazine d'argent et l'acide hyaluronique : une série de cas
Alison Carlin
DOI: 10.33235/wcet.44.1.36-39
Résumé
Les complications cutanées chez les stomisés sont largement répandues et peuvent entraîner des difficultés physiques et émotionnelles dans la vie de tous les jours. Les complications cutanées parastomiales chroniques peuvent être difficiles à cicatriser et provoquer des douleurs importantes.
Deux patients se sont présentés à la clinique de stomathérapie pour être traités et ont été diagnostiqués avec une ulcération cutanée parastomiale chronique. Après un traitement standard de la plaie, l'application d'une pommade corticostéroïde topique et l'examen de l'appareillage, les ulcères ne s'amélioraient pas ou réapparaissaient. Un traitement avec une crème combinée composée de 0,2 % d'acide hyaluronique (AH) et de 1 % de sulfadiazine d'argent (SSD) a été mis en place et les deux patients ont présenté une cicatrisation complète.
Le traitement de l'ulcération cutanée parastomiale à l'aide de la crème à double action 0,2 % d'AH et 1 % de SSD a été couronné de succès pour ces deux patients, avec une réduction de la douleur et du liquide purulent constatée tout au long du traitement, ainsi qu'une réduction du coût du traitement par rapport aux protocoles standard.
Introduction
Le risque qu'un stomisé développe une complication cutanée péristomiale au cours de sa vie a été estimé entre 6 % et 80 %1. Les stomisés souffrant d'une complication cutanée sont plus nombreux à avoir une image négative de leur corps2. Les hommes stomisés souffrant d'une complication cutanée étaient 1,72 fois plus susceptibles de déclarer une image corporelle négative que les stomisés ne souffrant d'aucune complication cutanée, et les femmes stomisées étaient encore plus nombreuses à déclarer une image corporelle négative, soit 1,87 fois plus2. Ces complications sont à l'origine d'environ 40 % de l’ensemble des visites aux infirmières et infirmiers stomathérapeutes3.
Les causes des complications cutanées péristomiales et parastomiales peuvent être complexes et inclure des lésions chimiques, des traumatismes cutanés, des infections, des dermatites de contact et des affections liées à la maladie4. Les complications cutanées péristomiales sont plus fréquentes chez les patients ayant une iléostomie (57 %) et une urostomie (48 %) que chez ceux ayant une colostomie (35 %)5. Bien que les complications cutanées péristomiales, y compris les ulcères, soient assez courantes, les ulcères parastomiaux chroniques sont inhabituels et peuvent être difficiles à prendre en charge6.
Les stomisés qui développent des ulcères parastomiaux souffrent souvent de pathologies sous-jacentes telles que la maladie de Crohn, la maladie du côlon irritable (MCI) ou le pyoderma gangrenosum (PG). Le traitement et la prise en charge d'un ulcère parastomial consistent en un examen de l'appareillage, des soins de la plaie, un traitement systémique (si le patient est atteint de la maladie de Crohn, d'une MCI ou d'un PG) et un traitement local, généralement un corticostéroïde6. Si un patient ne souffre pas de la maladie de Crohn, de MCI ou de PG, son ulcère parastomial est susceptible de réagir rapidement à un traitement local de la plaie6. Les symptômes comprennent souvent des douleurs, des difficultés d'appareillage et des fuites6. Souvent, ces ulcères ne semblent pas graves, mais les stomisés décrivent une forte douleur brûlante, exacerbée par les changements d'appareillage6.
Les complications cutanées associées aux stomies ont un impact considérable sur la qualité de vie des stomisés, et il est essentiel qu'elles soient résolues rapidement. L'objectif de cette étude de cas est d'examiner deux stomisés souffrant d'une ulcération parastomiale pour laquelle le protocole de traitement standard a échoué. Les stomisés ont ensuite testé un nouveau traitement combinant 0,2 % d'acide hyaluronique (AH) et 1 % de sulfadiazine d'argent (SDA).
Action du produit
L'AH induit une réaction de réparation tissulaire accélérée, caractérisée par la croissance d'un tissu de granulation bien organisé. La liaison des récepteurs de l'AH engage les cellules endothéliales, les macrophages, les fibroblastes et les kératinocytes et modifie leurs propriétés vers un état plus "orienté vers la réparation"7,8. Outre la stimulation des mécanismes de réparation cellulaire, l'importante capacité de liaison à l'eau des molécules d'AH offre des conditions idéales pour la migration et la reproduction des cellules qui forment de nouveaux tissus7,8.
Le SDA est une combinaison de deux agents antimicrobiens (argent et sulfadiazine) ayant des propriétés antibactériennes à large spectre et est particulièrement efficace contre les micro-organismes souvent présents dans les lésions cutanées infectées9. Appliqué sur des plaies exsudatives, le SDA libère ses ions d'argent qui augmentent l'effet bactériostatique du radical sulfamide. L'action antimicrobienne durable de l'association sulfadiazine-argent est due en partie à l'interaction continue avec les fluides sur le lit de la plaie, qui induit une libération lente et prolongée de l'argent9.
Il a été prouvé que le traitement combiné d'AH et de SDA (AH+SDA), comparé au SDA seul, accélère le processus de réparation tout en offrant une action antibactérienne à large spectre10. Des études cliniques ont démontré que l'utilisation du produit combiné AH+SDA permettait de réduire la durée des soins infirmiers, les dépenses et l'utilisation de médicaments contre la douleur11,12.
Présentations de cas
Cas 1
Le patient TW est une femme de 80 ans qui a subi une proctocolectomie totale avec formation d'une iléostomie terminale en mai 2020. L'iléostomie de la patiente était saine et la peau péristomiale est restée intacte jusqu'à ce qu'elle se présente à la clinique de jour de stomathérapie en juillet 2021 avec un ulcère d'étiologie inconnue. L'ulcère mesurait 80 mm x 50 mm et était adjacent à la stomie à 10 heures. Il n'y avait ni douleur ni odeur, l'exsudat était peu séreux et la base de la plaie était souple.
Prise en charge et résultats
Le traitement instauré le 22 juillet 2021 (Figure 1) consistait en une pommade aux corticostéroïdes, un pansement antibactérien à base d'argent et un pansement hydrocolloïde. Le pansement a été changé tous les jours en même temps que l'appareillage de stomie. Après un mois de traitement (Figure 2), la plaie mesurait 100 mm x 50 mm, avec une base propre et un liquide purulent. La peau péri-lésionnelle était fragile et risquait de se détériorer davantage. Le chirurgien colorectal de la patiente avait envisagé une biopsie pour exclure une infection de la plaie avec PG si la plaie continuait à ne pas montrer de signes d'amélioration.
Le traitement initial a été interrompu et un traitement avec une crème contenant 0,2 % d'AH et 1 % de SDA a été mis en place (AH+SDA). Le traitement était quotidien et s'accompagnait d'un changement d'appareillage de stomie, ce qui était la préférence de la patiente (Figure 3).
Après le traitement avec la crème AH+SDA, la taille de la plaie a continuellement diminué jusqu'à ce qu'elle soit cicatrisée. Il n'y avait ni douleur ni odeur et l'exsudat séreux a diminué. Le 16 septembre (Figure 4), le traitement a été interrompu et il a été conseillé au patient de reprendre le traitement en cas de réapparition de dégradation de la plaie ; cependant, la plaie a continué à cicatriser (Figure 5) et était toujours cicatrisée près de 12 mois plus tard.
Le coût du traitement standard par rapport au traitement combiné AH+SDA a montré des différences significatives (Figure 6). Le traitement combiné AH+SDA était plus de 40 % moins cher par changement de pansement, avec seulement 25 % du tube utilisé au total.
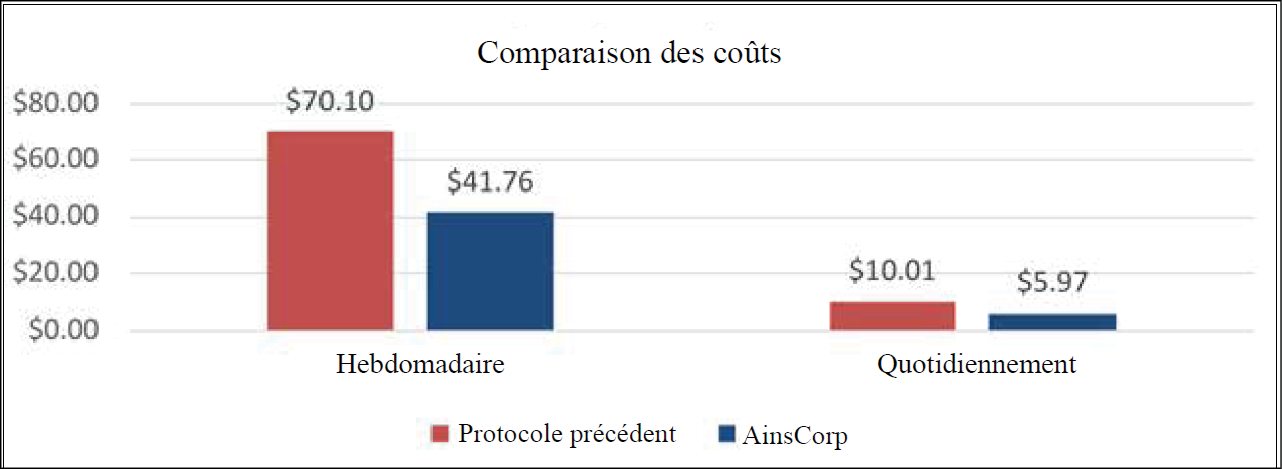
Figure 6. Cas 1 - comparaison des coûts du traitement standard et du traitement combiné AH+SDA sur une base hebdomadaire et quotidienne
Cas 2
Le patient ML est un homme de 84 ans à qui l'on a posé un conduit iléal en 2007. Le conduit iléal et la peau péristomiale du patient étaient sains après l'opération et n'avaient pas été examinés par un stomathérapeute depuis 11 ans. Le patient s'est présenté à la clinique ambulatoire de stomathérapie en juin 2021 avec une ulcération péristomiale et une perte de peau. L'ulcère mesurait 20 mm x 40 mm et s'étendait depuis le bord de la stomie de 12 heures à 7 heures. L'ulcère était extrêmement douloureux, avec une base visqueuse, un exsudat peu séreux, sans œdème ni odeur.
Prise en charge et résultats
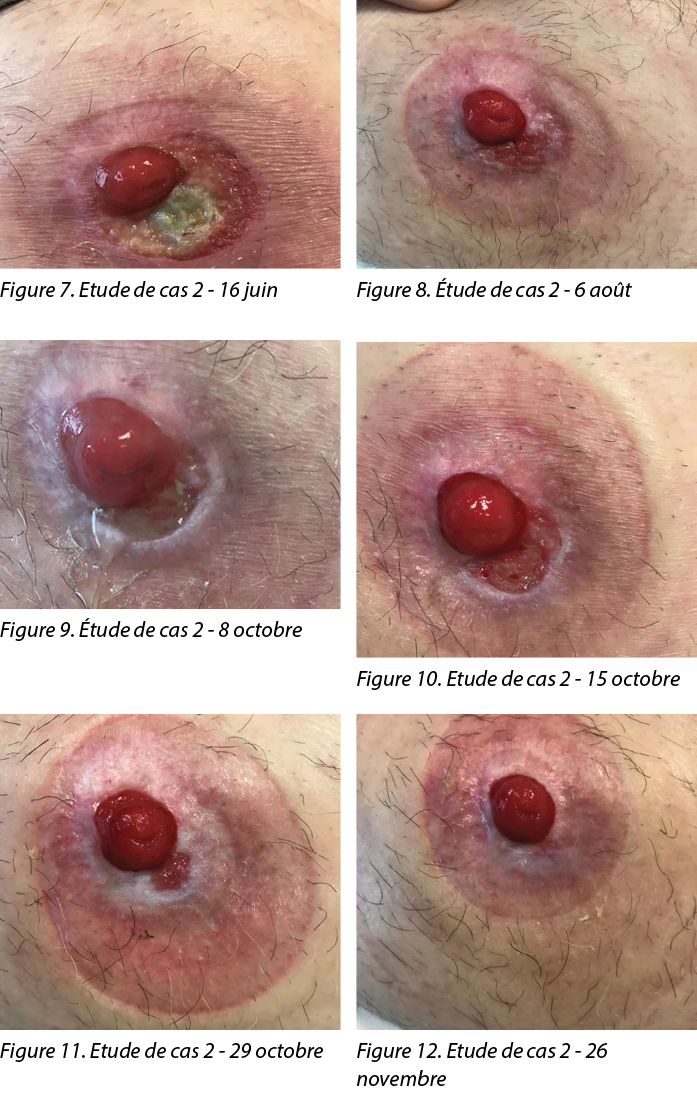
Le traitement initié le 16 juin 2021 (Figure 7) consistait en une pommade aux corticostéroïdes toutes les deux semaines, un pansement barrière antibactérien à l'argent et de joints de stomie hydrocolloïde petit et grand. Le pansement a été changé selon les préférences du patient et en cas de fuite de l'appareillage de stomie, ce qui variait d'une fois par jour à une fois par semaine.
Après 6 semaines de traitement (Figure 8), l'ulcère était cicatrisé et le traitement a été arrêté ; cependant, le nouveau tissu de granulation dans la partie de l'ulcère située entre 5 et 7 heures semblait très fragile. Le patient s'est à nouveau présenté le 8 octobre, l'ulcère s'étant à nouveau détérioré (Figure 9). La plaie mesurait 10 mm x 5 mm, avec une base pâle et visqueuse, une macération des bords de la plaie, un faible exsudat et aucune douleur, ni œdème ni odeur. À ce stade, le patient est revenu au régime de traitement initial, à savoir une pommade aux corticostéroïdes toutes les deux semaines, un pansement barrière antibactérien à l'argent et un joint de stomie hydrocolloïde. Le pansement a été changé tous les 2 ou 3 jours, en même temps que l'appareillage de stomie.
Après une semaine (Figure 10), la plaie s'est agrandie (10 mm x 20 mm), le traitement initial a été interrompu et un traitement avec une crème contenant 0,2 % d'AH et 1 % de SDA a été mis en place (AH+SDA). Le traitement était appliqué tous les deux jours en même temps que le changement de l'appareillage de stomie, selon les préférences du patient.
Après le traitement avec la crème AH+SDA, la taille de la plaie a continuellement diminué jusqu'à ce qu'elle soit cicatrisée. Deux semaines après le traitement initial (Figure 11), la plaie s’était réduite de 10 mm x 20 mm à 5 mm x 5 mm. Il y avait un tissu de granulation rose, un exsudat peu séreux et une certaine macération sur les bords de la plaie. Aucune douleur, œdème ou odeur n'a été constaté. Six semaines après le traitement (Figure 12), la plaie était cicatrisée et l'est toujours depuis.
Le coût du traitement standard par rapport au traitement combiné AH+SDA a montré des différences significatives (Figure 13). Le traitement combiné AH+SDAa permis de réduire de plus de 50 % le nombre de changements de pansements, avec seulement 25 % du tube utilisé au total.
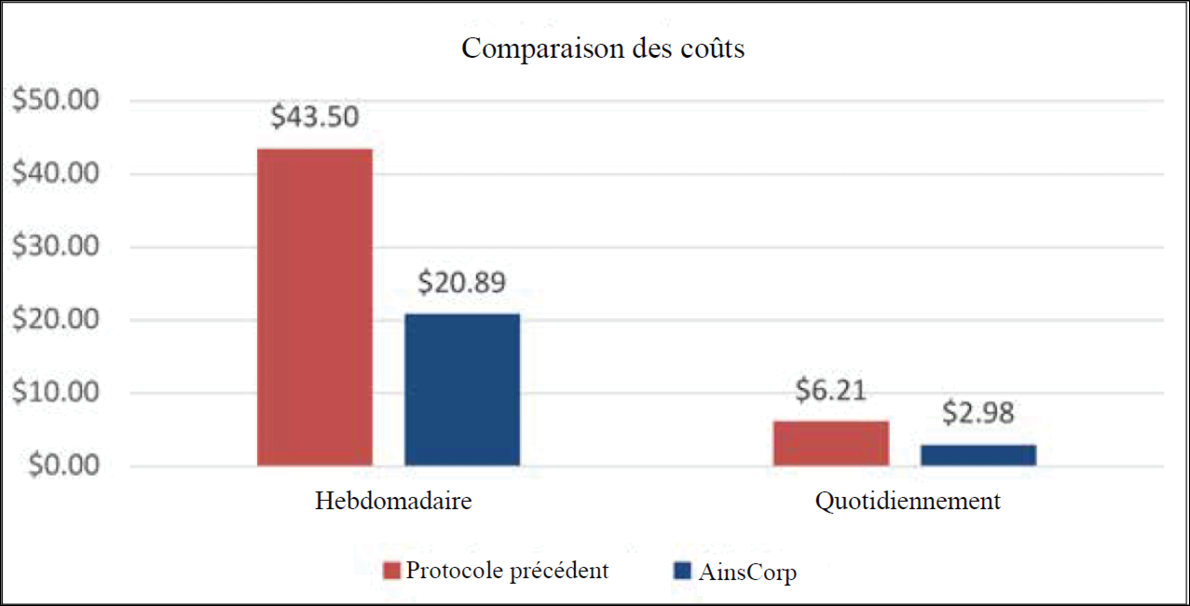
Figure 13. Cas 2 - comparaison des coûts du traitement standard et du traitement combiné AH+SDA sur une base hebdomadaire et quotidienne
Discussion
Les deux patients présentaient des ulcères parastomiaux d'étiologie inconnue qui ne se sont pas résorbés avec le traitement standard. Après le traitement avec la crème combinée 0,2 % d'AH et 1 % de SDA (AH+SDA), les ulcères ont été pris en charge et cicatrisés avec succès. Une quantité de crème combinée de la taille d'un petit pois a été appliquée en fine couche directement sur l'ulcère à l'aide d'un coton-tige, sans pansement secondaire, et l'appareillage de stomie a été appliqué par-dessus. L'application de crème sous la plaque de base n'a pas affecté l'adhérence de l'hydrocolloïde, et les deux patients n'ont pas signalé de fuite ou de soulèvement de la plaque de base avant le changement de poche. Ce traitement a facilité la sortie des patients de la clinique de stomathérapie, et les deux ulcères sont restés cicatrisés depuis.
Conclusion
Le coût du traitement standard par rapport au traitement combiné AH+SDA était significatif. Dans le cas 1, le coût du traitement standard était 1,68 fois plus élevé que celui du traitement combiné, et dans le cas 2, le coût du traitement standard était 2,08 fois plus élevé que celui du traitement combiné. En outre, le traitement standard a échoué pour les deux patients et les plaies n'étaient toujours pas cicatrisées après plusieurs semaines de traitement, alors que le coût du traitement combiné a été calculé en fonction du temps nécessaire à la cicatrisation des plaies. La différence de coût significative de la crème combinée AH+SDA par rapport au traitement standard des ulcères parastomiaux (sans tenir compte des examens supplémentaires du GP pour les scripts de Kenacomb®) indique qu'il pourrait s'agir d'une intervention efficace et peu coûteuse qui pourrait être appliquée dès la première présentation d'un ulcère parastomial.
Remerciements
Les patients ont consenti à l'utilisation de leurs données pour cette étude de cas. Les photographies ont été prises avec le consentement verbal et écrit des patients.
Conflit d'intérêt
Les auteurs ne déclarent aucun conflit d'intérêt.
Financement
Les auteurs n'ont reçu aucun financement pour cette étude.
Author(s)
Alison Carlin
Grad Cert Stomal Therapy Nursing
Stomal Therapy CNC
Knox Private Hospital, VIC, Australia
Email alison.carlin@healthscope.com.au
References
- Norman T, Haesler E, Carville K, et al. Establishing a consensus on stomal, parastomal and peristomal complications. J Stomal Therapy Aust 2022;42(2):10–19.
- Nichols TR, Riemer M. Body image perception, the stoma peristomal skin condition. Gastrointest Nurs 2011;9(1):22–26.
- Antonini M, Arena R, Mancini S, et al. Peristomal skin changes: what treatment should be adopted? Results of an observational multi-centre study. WCET J 2018;38(1):30–34.
- Taneja C, Netsch D, Rolstad BS, et al. Clinical and economic burden of peristomal skin complications in patients with recent ostomies. J Wound Ostomy Cont Nurs 2017;44(4):350–357.
- Herlufsen P, Olsen AG, Carlsen B et al. Study of peristomal skin disorders in patients with permanent stomas. J Wound Ostomy Cont Nurs 2013;40(4):400–6.
- Yeo H, Abir F, Longo WE. Management of parastomal ulcers. World J Gastroenterol 2006;12(20):3133–7.
- Chen CP, Hung W, Lin SH. Effectiveness of hyaluronic acid for treating diabetic foot: a systematic review and meta-analysis. Dermatol Ther 2014;27(6):331–6.
- Voigt J, Driver VR. Hyaluronic acid derivatives and their healing effect on burns, epithelial surgical wounds, and chronic wounds: a systematic review and meta-analysis of randomized controlled trials. Wound Repair Regen 2012;20(3):317–31.
- Farris A, Prosdocimi M, Bevilacqua C. Association of hyaluronic acid and silver sulphurdiazine for topical use: rational basis and recent clinical evidence in wound healing. Farmaci 2010;9(6):1–7.
- Costagliola M, Agrosi M. Second degree burns: a comparative, multicentre, randomized trial of hyaluronic acid plus silver sulfadiazine alone. Curr Med Res Opin 2005;21(8):1235–40.
- Soma PF, Stella M, Comitini S. Role of a HA based hyaluronic acid in re-epithelisation: a clinical model. 37th National Meeting of the Italian Society of Plastic, Reconstructive, and Aesthetic Surgery, 1988.
- Torregrossa F, Caroti A. Clinical trial of the topical use of hyaluronic acid-soaked gauzes in the treatment of sluggish ulcers. Giorn It Derm Vener 1983;118.