

Volume 40 Number 3
Successful treatment of an ileal conduit fistula with negative pressure: report of a case
Mengxiao Jiang, Huiming Lu, Meichun Zheng, Baojia Luo and Huiying Qin
Keywords negative pressure, dual tube, fistula of ileal conduit, urostomy
For referencing Jiang M et al. Successful treatment of an ileal conduit fistula with negative pressure: report of a case. WCET® Journal 2020;40(3):19-23.
DOI https://doi.org/10.33235/wcet.40.3.19-23
Abstract
Aim To present the management of a patient who developed a fistula from a uretero-ileostomy anastomosis of the ileal conduit by applying intra-conduit negative pressure through a dual tube.
Case report The patient was a 73-year-old man diagnosed with bladder cancer who underwent a radical cystectomy and formation of an ileal conduit in our centre. A fistula occurred in the ileal conduit less than 1 week after the surgery. Urine leaked continuously into the pelvic cavity which put the patient at risk of fluid and electrolyte imbalances. A further operation to suture the fistula to contain the leakage was suggested. To save the patient from a further operation, intra-conduit negative pressure through a dual tube was attempted to assist with management of the fistula. This conservative treatment promoted successful closure of the fistula.
Method It is clinically challenging to manage a urinary fistula associated with an ileal conduit in a conservative way. This is because the fistula is deep within the body cavity and it is almost impossible for the fistula to heal spontaneously. The literature reveals previous conservative treatment has been mostly unsuccessful. Surgical suturing of the fistula is the most used method but is not always an ideal choice. By applying intra-conduit negative pressure through a dual tube system to the ileal conduit, the aim was to facilitate closure of the fistula.
Conclusion In this case report the application of intra-conduit negative pressure through a dual tube to contain a fistula from a uretero-ileostomy anastomosis of an ileal conduit was found to be safe and effective. This method of conservative treatment is worth promoting.
Introduction
Bladder cancer is a highly prevalent disease associated with high recurrence and mortality1. Radical cystectomy is the gold standard treatment for both muscle invasive bladder cancer and recurrent high grade non-muscle invasive bladder cancer2. After radical cystectomy, surgeons mostly choose the formation of an ileal conduit or urostomy for urinary diversion3. It is reported that 15–16% of patients will develop a fistula within the conduit after urinary diversion4,5. Urinary fistula of an ileal conduit is a complex and serious complication that often occurs in the early postoperative period2,5. The occurrence of this complication will not only prolong the hospital stay of patients, but also increases the mortality rate5.
Management of a urinary fistula within an ileal conduit is difficult6. One management option to deal with this complication is further surgery to suture the fistula; however, operating twice on the patient in a short time can cause too much trauma. Doctors and ET nurses often feel very conflicted as to whether to operate a second time, especially when a patient’s physical and psychological condition may not be robust enough to tolerate secondary surgery. Further, the patient may refuse a second operation. In addition to surgical treatment, the literature reveals that other conservative management strategies such as percutaneous nephrostomy or a fenestrated conduit catheter usually fail to close the fistula5.
Negative pressure therapy is widely used to treat fistulas as it facilitates and accelerates drainage of fluid which increases the likelihood of the fistula healing7–9. Through a literature review, the authors found positive results in several patients with a fistula of an ileal conduit following the application of negative pressure therapy10,11. While these previous studies revealed that negative pressure therapy maybe a good clinical choice for managing a urinary fistula within an ileal conduit, these relevant reports are too few and more studies are needed to confirm the safety and efficacy of the treatment. Moreover, clinicians must be aware that ileal conduits are very vulnerable to secondary trauma during the negative therapy processes from the amount of negative pressure applied and catheter-related damage to the conduit5. In this case report, the authors present the outcome of the application of intra-conduit negative pressure in a patient with a fistula in a uretero-ileostomy anastomosis of an ileal conduit. The authors further demonstrate how to use a dual tube to decrease the treatment risk.
Case Presentation
A 73-year-old man in otherwise good health underwent a radical cystectomy and formation of an ileal conduit for muscle invasive bladder cancer. On the 5th postoperative day, the left pelvic drainage tube drained out 1350ml of faint yellow drainage, while the urinary stoma only drained out 700ml of urine. Urinary leakage of the intra-abdominal portion of the ileal conduit was suspected. Examination of fluid from the left pelvic drain confirmed the suspicion and presence of urine as creatinine was confirmed. The level of creatinine present in the drainage fluid was high at 4396.μmol/L – normal range of serum creatinine is 60–110μmol/L. A CT scan of the abdomen showed the fistula was located where the right transplanted ureter entered the ileal conduit.
Careful examination of the ileal conduit was also undertaken and a large amount of mucus was found to have accumulated in the ileal conduit. The doctor flushed the ileal conduit to clear the mucus away. However, although the ileal conduit was no longer obstructed from mucus, the urine still leaked into the pelvic cavity continuously. On the 6th postoperative day, the left pelvic drainage increased to 1890ml, while the urine draining out from the stoma decreased to 410ml. Urine leakage increased the risk of pelvic infection and water electrolyte imbalance; both clinical problems needed to be managed properly as soon as possible. A further operation to suture the fistula closed was suggested. However, taking the trauma of further surgery, the economic cost and the patient’s will into consideration, it was decided to attempt implementation of conservative treatment first.
Negative pressure therapy
The negative pressure system used was constructed by a doctor and an ET nurse. The authors chose this therapy with the aim of achieving two goals. Firstly to stop urine draining continuously into the pelvic cavity and secondly to promote the closure of fistula. A well-known contraindication is to apply negative pressure therapy to organs because the risk of traumatising organs is high. To avoid adverse events such as bleeding, ischaemia and catheter-related ileal conduit perforation from happening, the authors applied negative pressure to the ileal conduit through a dual tube (Figure 1). The dual tube consisted of a rigid tube and a soft tube. The rigid tube could conduct negative pressure well; however, it may cause mechanical damage to the ileal conduit. The soft tube was unable to sustain negative pressure but could protect the ileal conduit from catheter-related injuries by isolating the rigid tube from coming into contact with the ileal conduit. The steps used to construct and apply the therapeutic negative pressure system are listed as follows.
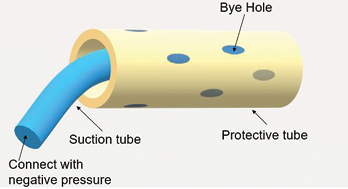
Figure 1. An illustration of a dual tube
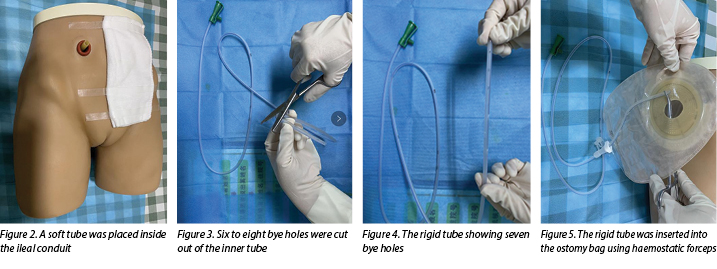
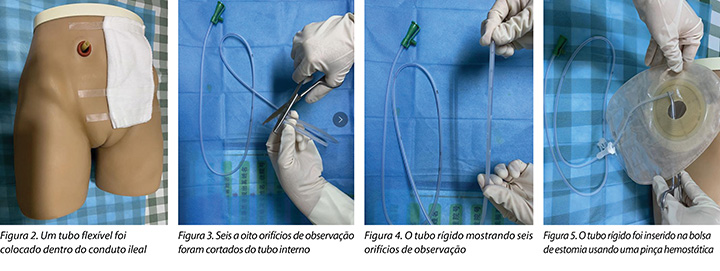
- Select a soft and protective medical latex tube as the outer tube. A soft tube is routinely placed inside the ileal conduit during operation and, as this tube had not been removed when the urinary fistula occurred in our case, it was used as the outer tube (Figure 2).
- Select a rigid tube such as a medical sputum aspiration tube as the inner tube.
- Cut six to eight bye holes out of the inner tube (Figures 3–4).
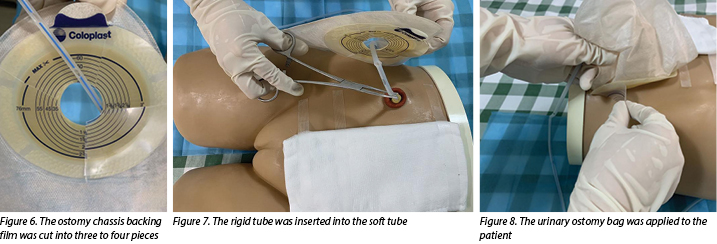
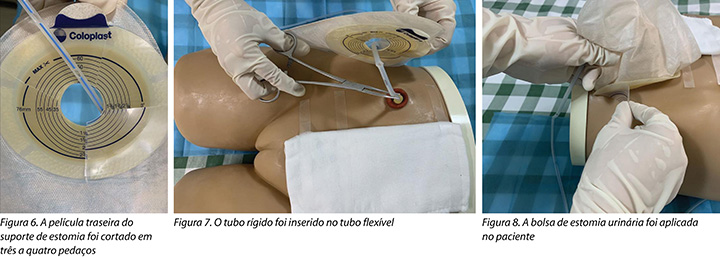
- Insert the rigid tube into the ostomy bag with haemostatic forceps (Figure 5), cut the ostomy chassis backing film into three to four pieces(Figure 6).
- The doctor then inserts a rigid tube into the soft tube (Figure 7). The insertion depth of the inner tube should be 1cm shorter than the outer tube.
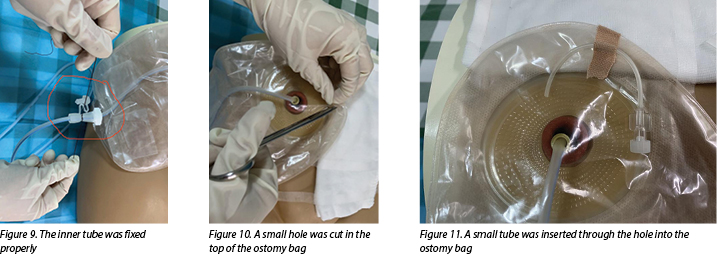
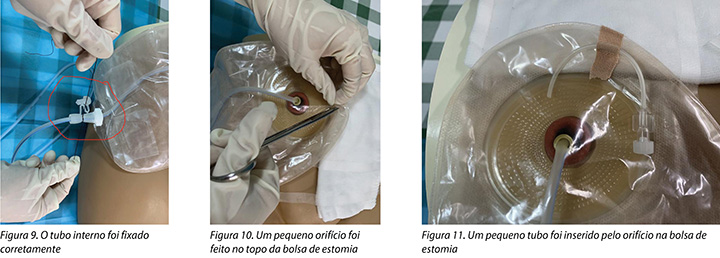
- Apply a urinary ostomy bag to the ostomy skin barrier or base plate (Figure 8) and fix the inner tube properly (Figure 9).
- Cut a small hole in the top of the ostomy bag (Figure 10), and insert a small tube through the hole into the ostomy bag to make the negative pressure semi-closed (Figure 11).
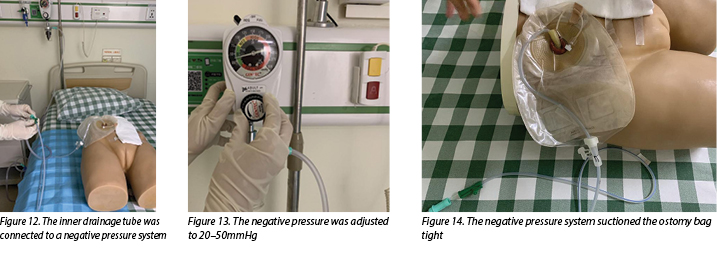
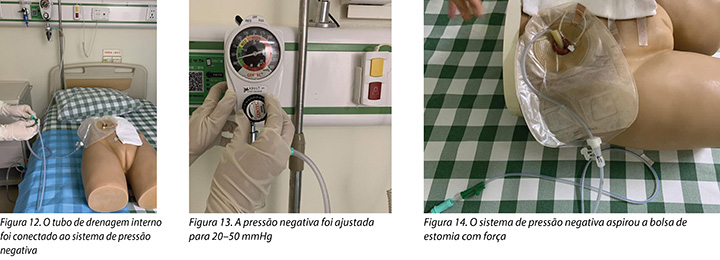
- Connect the inner drainage tube to a negative pressure system (Figure 12) and adjust the negative pressure to 20–50mmHg (Figure 13). In this case, wall suction was used, but a commercial negative pressure therapy machine is also suggested.
- After doing this, observe the negative pressure system suctioning the ostomy bag tight and, at the same time, urine should be immediately sucked out from the ileal conduit (Figure 14).
During the negative pressure therapy process, the patient’s fluid and electrolyte balance was closely monitored, the ileal conduit was cleared of mucus twice a day, and the patient was instructed to do passive activities while in bed. A nutritionist and psychotherapist were invited to join the medical, ET and nursing team to help improve the nutritional and psychological status of the patient.
After 12 days of negative pressure therapy treatment, the left pelvic drainage decreased to 210ml and the creatinine level of the drainage output was 73.7μmol/L, which indicated that urine was no longer leaking into the pelvic cavity. The negative pressure therapy was stopped 2 days later. It was pleasing to note that, following cessation of suction of the urine, there was no increase in pelvic drainage. The patient recovered well and was discharged from the hospital soon after. After a follow-up period of 3 months, no further anastomotic insufficiency was noted.
Discussion
While not a medical emergency, a fistula within an ileal conduit is a complication that is very difficult to manage conservatively. Up till now, the treatment of this type of fistula occurrence has still been in exploratory stages. Conservative management strategies such as percutaneous nephrostomy and fenestrated conduit catheters have been tried to manage these situations, but are reported to have a high failure rate5. Percutaneous nephrostomies are commonly used for urinary diversion, resulting in successful drainage of urine12; however, this method of urinary diversion does not aid fistula healing. Similarly, placing a fenestrated drainage tube or fenestrated catheter into an ileal conduit is also ineffective. While this method may increase the patency of urine drainage it does not prevent urine from leaking into the pelvic cavity, nor does it promote development of granulation tissue around the fistula to assist with fistula closure.
Proper drainage of urine and promotion of the growth of granulation tissue are keys factors for healing fistulas of this nature. Negative pressure systems can help stimulate the formation of granulation tissue and remove excess exudate away from the wound site13. Thus, negative pressure therapy may be a useful alternative for the treatment of urinary fistula. Continuous suction leads to the absorption of leaking urine and intestinal mucus that can cause infection and disturb fluid and electrolyte balance of the patient. In addition, stimulation of angiogenesis and granulation tissue formation increases the chance of fistula healing.
Although negative pressure appears to work well in promoting the closure of fistulas, it should be used and applied with caution to fistulas within an ileal conduit. Adverse events such as bleeding, ischaemia and intestinal perforation may occur due to using negative pressure therapy to exposed organs14. Safety is more important than a curative effect. Although no adverse events have been reported in previous studies10,11,15, this does not mean the therapy is safe and without risk. Some measures must be taken to decrease the treatment risk for the patient. Inserting a protective disc over the exposed organs could offer protection from local ischaemia, while still providing effective drainage16.
In the dual tube model discussed here, the outer tube acted as a protective disc, thereby protecting the ileal conduit from mechanical injury and decreasing the risk of ischaemia and haemorrhage that may be caused by negative pressure. An animal experiment showed negative pressure between 50–170mmHg caused a significant decrease in the microvascular blood flow in the intestinal loops16. The authors, therefore, adjusted the negative pressure to 20–50mmHg in this case to avoid ischaemia occurring. Compared with intestinal fistula, it was less likely that the suction tube would be obstructed when in a urinary fistula, so there was less need to adjust the negative pressure to more than 50mmHg. Moreover, keeping the negative pressure semi-closed was also a protective method to avoid ischaemia by stopping the tube from being tightly suctioned to intestinal tissue for long periods.
There are currently very few recommendations on the use of negative pressure therapy for the management of urinary fistula. As the patient did not have coagulation defects, the authors felt that, under close clinical observation, it would be worth trying very gentle negative pressure through a dual tube approach to aid urinary fistula healing. During the therapy process, it is necessary to regularly check whether the suction tube is displaced or obstructed, monitor the amount of the pelvic drainage and urine discharged in the collecting system of the device daily, and be alert for complications such as bleeding, ischaemia, infection and fluid and electrolyte imbalances. Urinary leakage at the anastomotic site of an ileal conduit can lead to periureteral fibrosis and scarring, thus predisposing to stricture formation6. Surgical follow-up to evaluate anastomotic status is also needed.
Summary
Fistula occurrence at the site of an ileal conduit is a serious complication after urostomy formation. How to promote the closure of urinary fistula quickly and effectively in a conservative way has been problematic and concerning for urologists and ET nurses for a long time. In this case report the authors have shared their successful experience with the application of negative pressure through a dual tube system to manage this complication. The treatment in this instance was found to be safe and effective. It is worth further exploration as the authors believe more patients could benefit from it.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
The authors received no funding for this study.
Tratamento bem sucedido de uma fístula de conduto ileal com pressão negativa: relato de caso
Mengxiao Jiang, Huiming Lu, Meichun Zheng, Baojia Luo and Huiying Qin
DOI: https://doi.org/10.33235/wcet.40.3.19-23
Resumo
Objetivo Apresentar o gerenciamento de um paciente que desenvolveu uma fístula a partir de uma anastomose de ureteroileostomia do conduto ileal aplicando pressão negativa intra-conduto através de um tubo duplo.
Relato de caso O paciente era um homem de 73 anos diagnosticado com câncer de bexiga e que passou por uma cistectomia radical e formação de um conduto ileal em nosso centro médico. A fístula ocorreu no conduto ileal menos de 1 semana após a cirurgia. A urina vazava continuamente na cavidade pélvica, colocando o paciente em risco de desequilíbrio de fluidos e eletrólitos. Sugeriu-se uma nova cirurgia para suturar a fístula e conter o vazamento. Para poupar o paciente de uma nova cirurgia, tentou-se a pressão negativa intra-conduto através de um tubo duplo para auxiliar no gerenciamento da fístula. Esse tratamento conservativo promoveu o fechamento da fístula com êxito.
Método O gerenciamento conservativo de uma fístula urinária associada a um conduto ileal é clinicamente desafiador. Isso ocorre porque a fístula está no fundo da cavidade do corpo e é quase impossível para a fístula ser recuperada espontaneamente. A literatura revela que tratamentos conservativos anteriores em sua maioria não tiveram êxito. A sutura cirúrgica da fístula é o método mais usado, mas nem sempre é a escolha ideal. Ao aplicar-se pressão negativa intra-conduto através de um sistema de tubo duplo ao conduto ileal, o objetivo é facilitar o fechamento da fístula.
Conclusão Neste relato de caso, a aplicação de pressão negativa intra-conduto por meio de um tubo duplo para conter a fístula de uma anastomose de ureteroileostomia de um conduto ileal foi segura e eficaz. Vale a pena promover esse método de tratamento conservativo.
Introdução
O câncer de bexiga é uma doença altamente prevalente associada à alta recorrência e mortalidade.1 A cistectomia radical é o tratamento padrão tanto para o câncer de bexiga invasivo muscular quanto para o câncer de bexiga recorrente não invasivo de alto grau.2 Após a cistectomia radical, a maioria dos cirurgiões escolhe a formação de um conduto ileal ou urostomia para o desvio urinário.3 Relata-se que 15 - 16% dos pacientes desenvolverão uma fístula dentro do conduto após o desvio urinário.4,5 A fístula urinária de um conduto ileal é uma complicação complexa e grave que geralmente ocorre no início do período pós-operatório.2,5 A ocorrência dessa complicação não só prolonga a estadia dos pacientes no hospital, como também aumenta a taxa de mortalidade.5
O gerenciamento de uma fístula urinária dentro de um conduto ileal é difícil.6 Uma opção de gerenciamento para lidar com essa complicação é a realização de uma nova cirurgia para suturar a fístula; no entanto, operar o paciente duas vezes em um curto período de tempo pode causar muito trauma. Médicos e estomaterapeutas muitas vezes ficam em conflito sobre uma nova cirurgia, principalmente quando a condição física e psicológica de um paciente pode não ser forte o suficiente para tolerar uma segunda cirurgia. Além disso, o paciente pode recusar uma nova cirurgia. Além do tratamento cirúrgico, a literatura revela que outras estratégias de gerenciamento conservativas, tais como a nefrostomia percutânea ou um cateter de conduto multi-perfurado, geralmente não conseguem fechar a fístula.5
A terapia por pressão negativa é amplamente usada para tratar fístulas, uma vez que facilita e acelera a drenagem do fluido, o que aumenta a probabilidade de reparação da fístula.7–9 Por meio de uma revisão de literatura, os autores encontraram resultados positivos em diversos pacientes com fístula de conduto ileal após a aplicação da terapia por pressão negativa.10,11 Embora esses estudos prévios tenham revelado que a terapia por pressão negativa possa ser uma boa opção clínica para o gerenciamento de uma fístula urinária dentro de um conduto ileal, esses relatos relevantes são escassos e mais estudos são necessários para confirmar a segurança e eficácia do tratamento. Além disso, os médicos devem estar cientes de que os condutos ileais são muito vulneráveis a traumas secundários durante os processos de terapia negativa devido à quantidade de pressão negativa aplicada e danos ao conduto relacionados ao cateter.5 Neste relato de caso, os autores apresentam o resultado da aplicação de pressão negativa intra-conduto em um paciente com fístula em uma anastomose de ureteroileostomia de um conduto ileal. Os autores demonstram ainda como usar um tubo duplo para diminuir o risco do tratamento.
Apresentação do caso
Um homem de 73 anos com boa saúde foi submetido a uma cistectomia radical e formação de um conduto ileal para câncer de bexiga invasivo muscular. No 5° dia do pós-operatório, o tubo de drenagem pélvico esquerdo drenou 1350 ml de um líquido amarelo claro, enquanto o estoma urinário só drenou 700 ml de urina. Suspeitou-se de vazamento urinário da porção intra-abdominal do conduto ileal. O exame do líquido do dreno pélvico esquerdo confirmou a suspeita e a presença de urina assim que a creatinina foi confirmada. O nível de creatinina presente no fluido de drenagem estava alto em 4396 .μmol/L – a variação normal da creatinina sérica é 60-110 μmol/L. Uma tomografia computadorizada do abdome mostrou que a fístula estava localizada onde o ureter direito transplantado entrava no conduto ileal.
Um exame cuidadoso do conduto ileal também foi realizado e descobriu-se uma grande quantidade de muco acumulado no conduto ileal. O médico enxaguou o conduto ileal para limpar o muco. No entanto, embora o conduto ileal não estivesse mais obstruído pelo muco, a urina ainda vazava para a cavidade pélvica continuamente. No 6º dia do pós-operatório, o dreno pélvico esquerdo aumentou para 1890 ml, enquanto a urina drenada do estoma diminuiu para 410 ml. O vazamento de urina aumentou o risco de infecção pélvica e desequilíbrio de eletrólito de água; ambos problemas clínicos precisavam ser gerenciados adequadamente o mais rápido possível. Sugeriu-se uma nova operação para suturar a fístula. No entanto, levando em consideração o trauma de uma nova cirurgia, o custo e o desejo do paciente, decidiu-se primeiro fazer uma tentativa de implementação de um tratamento conservativo.
Terapia por pressão negativa
O sistema de pressão negativa usado foi construído por um médico e um estomaterapeuta. Os autores escolheram essa terapia procurando atingir dois objetivos. Em primeiro lugar, para impedir a drenagem contínua da urina para a cavidade pélvica e, em segundo lugar, para promover o fechamento da fístula. Uma contraindicação bem conhecida é aplicar a terapia por pressão negativa em órgãos, pois o risco de traumatizar os órgãos é alto. Para evitar a ocorrência de eventos adversos, tais como sangramento, isquemia e perfuração do conduto ileal relacionada ao cateter, os autores aplicaram pressão negativa no conduto ileal por meio de um tubo duplo (Figura 1). O tubo duplo consistiu em um tubo rígido e um tubo flexível. O tubo rígido poderia conduzir a pressão negativa bem; no entanto, podia causar dano mecânico ao conduto ileal. O tubo flexível não era capaz de sustentar a pressão negativa, mas poderia proteger o conduto ileal de lesões relacionadas ao cateter, isolando o tubo rígido do contato com o conduto ileal. Os passos usados para construir e aplicar o sistema de terapia por pressão negativa estão listados abaixo.
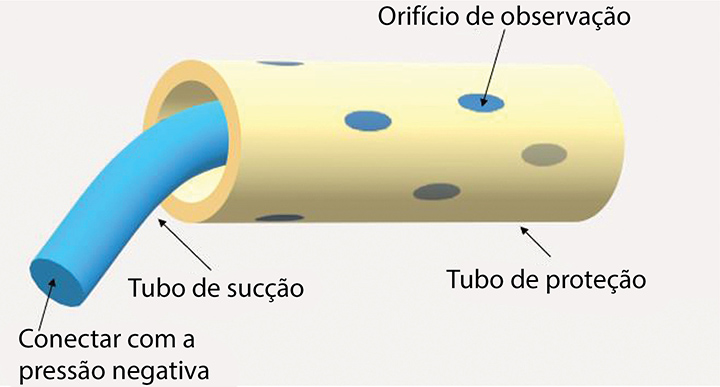
Figura 1. Uma ilustração de um tubo duplo
- Selecione um tubo de látex médico flexível e protetor como tubo externo. Um tubo flexível é rotineiramente colocado dentro do conduto ileal durante a cirurgia e, como esse tubo não havia sido removido quando a fístula urinária ocorreu em nosso caso, ele foi usado como tubo externo (Figure 2).
- Selecione um tubo rígido, como um tubo médico de aspiração de escarro, como tubo interno.
- Corte de seis a oito orifícios de observação do tubo interno (Figuras 3–4).
- Insira o tubo rígido na bolsa de estomia com uma pinça hemostática (Figura 5), corte a película traseira do suporte de estomia em três a quatro pedaços (Figura 6).
- O médico então insere um tubo rígido no tubo flexível (Figura 7). A profundidade de inserção do tubo interno deve ser 1 cm menor do que o tubo externo.
- Aplique uma bolsa de estomia urinária à barreira de pele da estomia ou placa base (Figura 8) e afixe o tubo interno adequadamente (Figura 9).
- Corte um pequeno buraco no topo da bolsa de estomia (Figura 10) e insira um pequeno tubo pelo buraco até a bolsa de estomia para tornar a pressão negativa semifechada (Figura 11).
- Conecte o tubo de drenagem interno ao sistema de pressão negativa (Figura 12) e ajuste a pressão negativa para 20–50 mmHg (Figura 13). Neste caso, uma parede de sucção foi usada, mas também sugere-se uma máquina de terapia por pressão negativa comercial.
- Feito isso, observe o sistema de pressão negativa aspirando a bolsa de estomia bem apertado e, ao mesmo tempo, a urina deve ser sugada imediatamente do conduto ileal (Figura 14).
Durante o processo de terapia por pressão negativa, o equilíbrio de fluido e eletrólito do paciente foi monitorado atentamente, o conduto ileal foi limpo de muco duas vezes ao dia e o paciente foi instruído a fazer atividades passivas enquanto estava deitado. Um nutricionista e um psicoterapeuta foram convidados a se juntar à equipe de médicos, estomaterapeutas e enfermeiros para ajudar a melhorar a situação nutricional e psicológica do paciente.
Após 12 dias de tratamento de terapia por pressão negativa, o dreno pélvico esquerdo diminuiu para 210 ml e o nível de creatinina do dreno de saída foi 73,7 μmol/L, indicando que a urina não estava mais vazando para a cavidade pélvica. A terapia por pressão negativa foi interrompida 2 dias depois. Foi bom notar que, após a interrupção da sucção da urina, não houve aumento na drenagem pélvica. O paciente se recuperou bem e teve alta hospitalar logo em seguida. Após um período de acompanhamento de 3 meses, nenhuma outra insuficiência anastomótica foi observada.
Discussão
Embora não seja uma emergência médica, uma fístula em um conduto ileal é uma complicação que é muito difícil de ser gerenciada de forma conservativa. Até agora, o tratamento desse tipo de fístula ainda se encontra em estágios exploratórios. Estratégias conservativas de gerenciamento, tais como nefrostomia percutânea e cateteres de conduto multi-perfurados, foram testadas para gerenciar essas situações, mas relataram ter um alto índice de falha.5 Nefrostomias percutâneas são comumente usadas para o desvio urinário, resultando na drenagem bem sucedida da urina12; no entanto, esse método de desvio urinário não ajuda na reparação da fístula. Da mesma forma, colocar um tubo de drenagem ou cateter multi-perfurado no conduto ileal também é ineficaz. Embora esse método possa aumentar a permeabilidade da drenagem da urina, ele não impede que a urina vaze para a cavidade pélvica, nem promove o desenvolvimento de tecido de granulação ao redor da fístula para auxiliar em seu fechamento.
A drenagem adequada da urina e a promoção do crescimento do tecido de granulação são os fatores principais para a reparação de fístulas dessa natureza. Sistemas de pressão negativa podem ajudar a estimular a formação de tecido granular e remover o excesso de exsudato do local da ferida.13 Portanto, a terapia por pressão negativa pode ser uma alternativa útil para o tratamento da fístula urinária. A sucção contínua leva à absorção da urina e do muco intestinal que podem causar infecção e perturbar o equilíbrio de fluidos e eletrólitos do paciente. Além disso, a estimulação da angiogênese e a formação do tecido de granulação aumentam a chance de reparação da fístula.
Embora a pressão negativa aparente funcionar no fechamento de fístulas, ela deve ser usada e aplicada com cuidado nas fístulas de um conduto ileal. Eventos adversos, como sangramento, isquemia e perfuração intestinal, podem ocorrer devido ao uso de terapia por pressão negativa em órgãos expostos.14 A segurança é mais importante do que um efeito curativo. Embora nenhum evento adverso tenha sido relatado em estudos anteriores10,11,15, isso não significa que a terapia é segura e não apresenta riscos. Algumas medidas devem ser tomadas para diminuir o risco do tratamento para o paciente. A inserção de um disco protetor sobre os órgão expostos pode oferecer proteção contra isquemia local, ao mesmo tempo em que fornece uma drenagem eficaz.16
No modelo com dois tubos discutido aqui, o tubo externo serviu como um disco protetor, protegendo assim o conduto ileal de lesões mecânicas e diminuindo o risco de isquemia e hemorragia que podem ser causadas pela pressão negativa. Um experimento com animais mostrou que a pressão negativa entre 50-170 mmHg causou uma diminuição significativa no fluxo sanguíneo microvascular nas alças intestinais.16 Os autores, portanto, ajustaram a pressão negativa para 20–50 mmHg nesse caso para evitar uma isquemia. Comparado com a fístula intestinal, é menos provável que o tubo de sucção seja obstruído em uma fístula urinária, então não havia necessidade de ajustar a pressão negativa para mais de 50 mmHg. Ademais, manter a pressão negativa semifechada também foi um método protetor para evitar uma isquemia, impedindo que o tubo fosse fortemente aspirado para o tecido intestinal por longos períodos.
Atualmente há poucas recomendações no uso de terapia por pressão negativa para o gerenciamento de fístulas urinárias. Como o paciente não apresentava defeitos de coagulação, os autores acharam que, sob observação clínica cuidadosa, valeria a pena tentar uma pressão negativa muito suave por meio de uma abordagem de tubo duplo para ajudar na reparação da fístula urinária. Durante o processo de terapia, é necessário verificar regularmente se o tubo de sucção está fora do lugar ou obstruído, monitorar diariamente a quantidade de drenagem pélvica e urina liberadas no sistema coletor do dispositivo e estar atento a complicações, tais como sangramento, isquemia, infecção e desequilíbrio de fluido e eletrólitos. O vazamento de urina no local anastomótico de um conduto ileal pode levar à fibrose periureteral e cicatrizes, predispondo assim a formação de estenose.6 O acompanhamento cirúrgico para avaliar o estado da anastomose também é necessário.
Resumo
A ocorrência de fístula no local de um conduto ileal é uma complicação grave após a formação de uma urostomia. Como promover o fechamento da fístula urinária de forma rápida, eficaz e conservativa tem sido um fator problemático e preocupante para urologistas e estomaterapeutas há muito tempo. Neste relato de caso, os autores compartilharam sua experiência bem sucedida na aplicação de pressão negativa por um sistema de tubo duplo para gerenciar essa complicação. O tratamento neste caso foi considerado seguro e eficaz. Vale a pena explorar mais esse tópico, pois os autores acreditam que mais pacientes poderiam se beneficiar com isso.
Conflito de interesse
Os autores declaram não haver conflitos de interesse.
Financiamento
Os autores não receberam financiamento para este estudo.
Author(s)
Mengxiao Jiang
MD
Department of Urology Surgery; Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China; Collaborative Innovation Center for Cancer Medicine
Huiming Lu
BD
Department of Urology Surgery; Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China; Collaborative Innovation Center for Cancer Medicine
Meichun Zheng
BD
Department of Colorectal Surgery; Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China; Collaborative Innovation Center for Cancer Medicine
Baojia Luo
MD
Department of Colorectal Surgery; Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China; Collaborative Innovation Center for Cancer Medicine
Huiying Qin*
MD
Department of Nursing Division, Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China; Collaborative Innovation Center for Cancer Medicine
Email qinhy@sysucc.org.cn
* Corresponding author
References
- Sanli O, Dobruch J ,Knowles MA, et al. Bladder cancer. Nat Rev Dis Primers, 2017;3:17022. doi:10.1038/nrdp.2017.22
- Wei ST, Lamb BW, Kelly JD. Complications of radical cystectomy and orthotopic reconstruction. Adv Urol 2015;2015(3):1-7. doi:10.1155/2015/323157.
- Kotb A F. Ileal conduit post radical cystectomy: modifications of the technique. J Ecancermedicalscience 2013;7:301.
- Teixeira SC, Ferenschild FT, Solomon MJ, et al. Urological leaks after pelvic exenterations comparing formation of colonic and ileal conduits. Eur J Surg Oncol 2012;38(4):361–366.
- Brown KG, Koh CE, Vasilaras A, et al. Clinical algorithms for the diagnosis and management of urological leaks following pelvic exenteration. Eur J Surg Oncol 2014;40(6):775–781.
- Farnham SB, Cookson MS. Surgical complications of urinary diversion. World J Urol 2004;22(3):157–167.
- Bobkiewicz A, Walczak D, Smolinski S, et al. Management of enteroatmospheric fistula with negative pressure wound therapy in open abdomen treatment: a multicentre observational study. Int Wound J 2017;14(1):255–264.
- Ruiz-Lopez M, Titos A, Gonzalez-Poveda I, et al. Negative pressure therapy as palliative treatment for a colonic fistula. Int Wound J 2014;11(2):228–229.
- Loaec E, Vaillant PY, Bonne L, et al. Negative-pressure wound therapy for the treatment of pharyngocutaneous fistula. Eur Ann Otorhinolaryngol Head Neck Dis 2014;131(6):351–355.
- Yetişir F, Salman AE, Aygar M, et al. Management of fistula of ileal conduit in open abdomen by intra-condoit negative pressure system. Int J Surg Case Rep 2014;5(7):385–388.
- Denzinger S, Luebke L, Burger M, et al. Vacuum-assisted closure therapy in ureteroileal anastomotic leakage after surgical therapy of bladder cancer. World J Surg Oncol 2007;5(1):41.
- Ahmad I, Pansota MS. Comparison between double J (DJ) ureteral stenting and percutaneous nephrostomy (PCN) in obstructive uropathy. Pakistan J Med Sci 2013;29(3):725–729.
- Wolvos T. The evolution of negative pressure wound therapy: negative pressure wound therapy with instillation. J Wound Care 2015;24(4 Suppl):15–20.
- Ontario HQ. Negative pressure wound therapy: an evidence update. Ontario Health Technology Assessment 2010;10(22):1.
- Heap S, Mehra S, Tavakoli A, et al. Negative pressure wound therapy used to heal complex urinary fistula wounds following renal transplantation into an ileal conduit. Am J Transplant 2010;10(10):2370–2373.
- Lindstedt S, Hlebowicz J. Blood flow response in small intestinal loops at different depths during negative pressure wound therapy of the open abdomen. Int Wound J 2013;10(4):411–417.

