

Volume 25 Number 4
Subjective wellbeing amongst informal caregivers of people with wounds: a cross-sectional survey
Katherine Rich and Dominic Upton
Keywords wounds, Informal caregiving, caregiver burden, subjective wellbeing
Abstract
Objective: The present study investigated subjective wellbeing amongst informal caregivers of people with wounds. Although under-investigated in the wound care literature, prior research indicates that informal caregiving results in a series of poorer outcomes for the caregiver.
Methods: A convenience sample of 57 caregivers (16 male, 41 female, 19–84 years old), was recruited from public outpatient facilities. Participants completed measures of caregiving satisfaction, and subjective wellbeing, in addition to characteristics about themselves and the care provided.
Results: The informal caregivers of people with wounds scored significantly lower on a measure of subjective wellbeing than the Australian population to a large effect (d = 1.11). Negative associations were identified between sleep and subjective wellbeing, while positive associations were found between caregiving satisfaction, and relationship quality with subjective wellbeing.
Discussion: Caregivers displayed lower subjective wellbeing than the general population. Subjective wellbeing was related to sleep, satisfaction, and relationship quality. Future research should compare outcomes of the caregivers of people with different forms of wounds, and should determine if correlating stressors and mediators are causal to wellbeing.
Background
Chronic and non-healing wounds are common, with estimates suggesting 400,000 people are living with these types of wounds in Australia1,2. These wounds may impact on the patient’s mobility, ability to complete tasks of daily living, social functioning, and can cause considerable psychosocial difficulties3-5. Accordingly, persons living with hard-to-heal wounds require different levels of assistance from formal caregivers, in partnership with, or exclusively by informal caregivers2,6. Informal caregivers are usually family members (although they may be a friend or neighbour), and can provide assistance with: activities of daily living, psychological support, attending medical appointments, or a component of the care recipient’s treatment7,8. Little research is available regarding those informally caring for someone with a wound, including estimates of how many exist in Australia, although literature focusing on the caregivers of other conditions indicates the role can result in significant costs to the caregiver9-11.
The existent research regarding informal caregivers of people with wounds has indicated this population experiences a similar intensity of burden as demonstrated amongst caregivers of other conditions4,12. Key areas of impact amongst this population have been established as: increases in stress, fear, and isolation4,12. This is in contrast to the broader informal caregiving research, which found burden primarily impacted: psychological, physical, financial, and social outcomes7. Furthermore, there is some indication provided by an integrative literature review, that informal caregivers of people living with wounds have identified a need for increases in the information and training they are provided about the subject of their care’s treatment6. Although the findings of studies have revealed similar themes between caring for a person with a wound and other conditions, the current research has not allowed for a comprehensive understanding of the consequences of informally caring for people with wounds2. Thus, with the available research, interventions to maximise the health and positive outcomes for these caregivers cannot be determined.
Within the caregiving literature, subjective wellbeing is one variable that has been used to measure caregiver outcomes. Subjective wellbeing is a cognitive and affective construct, measuring ratings of positivity about oneself, and about one’s life13,14. Subjective wellbeing, as represented by the theory of homeostatic wellbeing, is suggested to remain stable under normal conditions; however, under prolonged stressful circumstances it may be negatively influenced13,15. A large-scale study of Australian informal caregivers provided support for this theory and indicated informal caregiving may be considered a prolonged stressful circumstance, with these caregivers scoring significantly lower than the general population15.
While the research indicates there are psychosocial costs associated with informal caregiving, there is evidence suggesting these outcomes may be influenced by other individual factors16-19. This has been best described by the Stress Process Model, which suggests the combination of personal characteristics, context, stressors, and mediators all play a significant role in the consequences for an informal caregiver17. Support for this model has been evident throughout the caregiving literature16-20. In essence, this model does not suggest that a single factor, or the overall role, is the most influential towards caregiver outcomes; instead that some combination of these factors may be more protective against poor outcomes than others17.
Aim and Hypothesis
The aim of the present study was to determine if the subjective wellbeing amongst the informal caregivers of people living with wounds differs from the general Australian population, and to explore factors which relate to wellbeing amongst these caregivers. It was hypothesised in accordance with previous literature that this population of informal caregivers would score lower on subjective wellbeing than the general Australian population. The literature indicates outcomes for informal caregivers may be influenced by other factors that have been suggested as having stressful or mediating effects on a caregiver’s wellbeing. These factors were included to assess if any such relationships were present. Therefore, it was hypothesised that the variables considered to be stressors would have a negative relationship with subjective wellbeing, and the variables considered to be mediators would have a positive relationship with subjective wellbeing.
Method
Participants and exclusion criteria
The participants were recruited via convenience sample over a period of two months, from public outpatient care services, where the care recipient was receiving formal care for their wound. The participating facilities included the ambulatory care clinics of five community health centres, in addition to the vascular and high-risk podiatry clinics at a hospital within the Canberra region. To be eligible for participation, the person providing the care was required to be over the age of 18, and providing informal care to a person currently living with a wound. Persons who did not meet this criteria were excluded. For the purpose of this study, informal caregiving was defined as any amount of physical, psychological or task-based support, that one person provided to another due to illness or disease.
Measures
Caregiver characteristics. Three items were created to measure caregiver characteristics, including the participant’s age, gender, and employment status.
Stressors. Three open response items were devised to measure stressors. These items included: the time the wound had been present in months, the time the caregiver had been caring for the recipient in total, and how many hours per week the caregiver provided care overall (not specific to wound care). Three restricted response items were created for the purpose of the study to measure additional stressors, including: frequency with which sleep was disturbed due to caregiving, number of dependants (excluding the person with the wound), and reductions to leisure time as a result of caregiving.
Mediators. One open response item measured how many hours per week the caregiver engaged in leisure activities. Two items created for the purpose of this study measured the caregiver’s perceived relationship quality with the care recipient across a 5-point Likert scale (1 = low quality, 5 = high quality), with higher scores representing higher perceived relationship quality. This item first asked the caregiver to reflect on the quality of their relationship prior to the wound's development. They were then asked to rate the current quality of the relationship.
A fourth mediating variable was measured utilising the Revised Caregiving Satisfaction Scale (RCSS)21. The scale had six items, measured on a 5-point Likert scale (Five of the items: 1 = never, 5 = nearly always. One item: 1= disagree a lot, 5 = agree a lot)21. For the present study, the scale was modified, replacing the term ‘elder’ with ‘person you are caring for’. The items of the scale measured global satisfaction in the role, and the role's effects on improving: self-esteem, pleasure, feelings of closeness, meaning in life, and enjoying time with the recipient21,22. The six items were summed, with a resulting scale, which ranged between 6 and 30, with higher scores indicating higher feelings of satisfaction in the caregiving role21. Internal consistency was found similar to previous research with a Cronbach’s alpha at .89 in the present study, comparable to .87 found previously21.
Subjective wellbeing. To measure subjective wellbeing, the International Wellbeing Group’s (2013) Personal Wellbeing Index (PWI) — Adult (5th edition) was employed. Participants rated their satisfaction across seven life domains, allowing for a global estimate of the individual’s subjective wellbeing23. On each domain, the participants responded to one item, asking them to rate their satisfaction on an 11-point Likert scale (0 = no satisfaction at all, 10 = completely satisfied). For example: "How satisfied are you with your standard of living?"23. The scores of all seven items were then averaged, and multiplied by 10. The scale had a range of 10 to 100, with higher scores indicating higher levels of subjective wellbeing23. Internal consistency was found to be satisfactory in the present study, with a Cronbach’s alpha of .88. This was comparable to previous uses of the scale internationally, which has found Cronbach’s alpha to fall between .70 and .8523.
Procedure and design
Due to the hard to research population and privacy concerns, the study comprised of a cross-sectional survey design. Cross-institutional ethics approval was obtained from the Human Research Ethics Committee of The University of Canberra, and The ACT Health Human Research Ethics Committee (HREC 16-97; ETHLR.16.096). Participants were recruited and provided with the questionnaire pack via three methods: approached at the clinic directly, the care recipient was approached at the clinic and provided a questionnaire pack to give to their caregiver, or approached at a home visit solely by the nursing team. Permission for the researcher to make contact at the clinic was first sought by the health care teams. The questionnaire pack comprised of an information sheet with the researcher’s contact details, a consent form, the questionnaire, and a postage-paid envelope for return.
Participants were informed that the purpose of the project was to investigate the satisfaction and wellbeing of people providing informal care to people living with wounds, and that the voluntary survey was anticipated to take five to 10 minutes to complete. Informed consent was obtained. Flexibility was provided to participants, who chose when and where their participation occurred. The participants were informed collection boxes were provided at reception, or could be returned directly to the researcher if completed at the clinic, or via the provided postage-paid envelope.
Results
Demographic characteristics
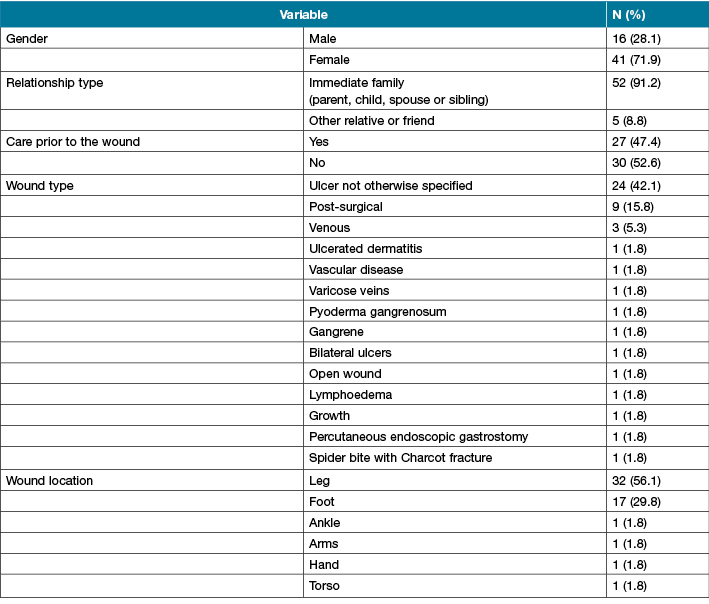
Demographic characteristics of the sample can be seen in Table 1. Of the 90 caregivers invited, 57 chose to participate in the study, with a response rate of 63%. This was large when compared to the response rate of 37% that occurred on a large-scale study of informal caregiver wellbeing15. The participants were aged between 19 and 84 years old (M = 58.91, SD = 15.48), and the majority were caring for an immediate family member. Almost half of the sample (47.4%) was providing informal care for the person with the wound prior to the wound's development. This indicated these participants were providing care for someone with co-morbid health conditions, possibly related to the wound's aetiology. However, the reason for prior care was not recorded. No information was recorded on those who choose not to participate for privacy reasons.
Table 1: Participant demographics (n=57)
Data screening and recoding
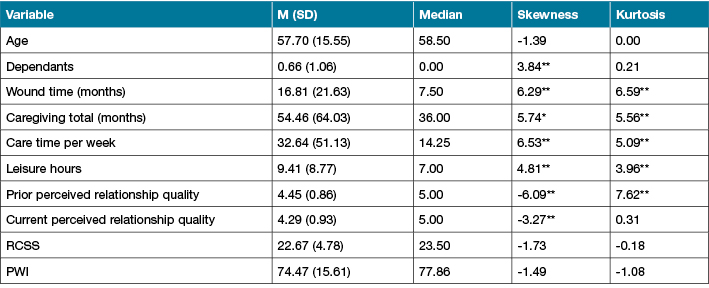
Data screening revealed some violations to normality (Table 2) and these violations were managed using non-parametric statistics, where appropriate. Six cases were then removed in accordance with the PWI manual for extreme responding (responses for all items as 0 or 10)22. An inspection of the z-scores revealed three extreme univariate outliers that exceeded the z value of +/– 3.3. Of these outliers, two remained within the realistic and possible range of scores and were retained for further analysis. The remaining outlier was identified to be caregiving for 33.3 years longer than the next highest case, and was also found to have missing data across four of the 30 items (13.3%). Due to this, the case was removed.
Table 2: Descriptive statistics of the continuous variables, including standardised skewness and kurtosis scores (n=50)
Subjective wellbeing
A one sample z-test was used to compare the sample mean (M = 74.5, SD = 15.79) and the Australian normed value of subjective wellbeing (M =75.3, SD = 0.72)23. The analysis revealed significant results (z = 7.86, p < .001, two-tailed), indicating the subjective wellbeing amongst the sample of informal caregivers of people with wounds was significantly lower than the general Australian population, to a large effect (d = 1.11), 95% CI [74.49, 75.10].
Factors relating to subjective wellbeing
Spearman’s rank-order correlation coefficient was used to determine if monotonic relationships were present between subjective wellbeing and the predictor variables. Of the variables tested, four of the predictor variables were found to have a significant relationship with subjective wellbeing (Table 3). Sleep was found to have a significant negative relationship with subjective wellbeing, ρ = –.34, N = 48, p < .05. Perceived relationship quality ratings at time of testing, ρ = .45, N = 48, p <.001, and prior to the wound, ρ = .35, N = 48, p < .05, had significant positive relationships with subjective wellbeing. Caregiving satisfaction was also found to have a significant positive relationship with subjective wellbeing ratings, ρ = .30, N = 48, p < .05.
Table 3: Bias corrected and accelerated correlations between predictor variables and subjective wellbeing based on 1000 bootstraps (n=48)
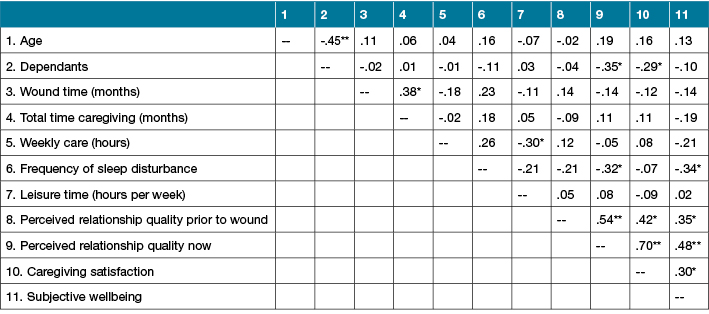
Four additional correlations were found amongst the predictor variables worthy of note. Caregiving satisfaction had significant positive correlations with both relationship quality at the time of testing, ρ = .70, N = 48, p < .001, and perceptions of quality retrospective to the wound, ρ = .42, N = 48, p < .05. A significant positive correlation was also identified between perceptions of relationship quality prior to the wound, and of the relationship on the day of testing, ρ = .54, N = 48, p < .001.
Discussion
The aim of the present study was to investigate subjective wellbeing amongst the informal caregivers of people living with wounds. The initial hypothesis predicted subjective wellbeing scores would be lower amongst this population than the Australian normed values. This was supported by the analysis to a large effect size, and was consistent with previous research findings comparing informal caregivers with the general population of Australians across the same measure14. In terms of the theory of homeostatic wellbeing, the finding indicates that caring for a person with a wound significantly differs from normal life circumstances inasmuch as it is likely caring for a person with a wound constitutes a perpetually stressful circumstance14.
The second hypothesis predicted stressor variables would have a negative association with wellbeing, and mediating variables would have a positive association with wellbeing. This was partially supported in the present study, with only four of the predictor variables having significant relationships with subjective wellbeing. Of these variables, one stressor (sleep), was identified to have a negative relationship with subjective wellbeing, and three mediators (care giving satisfaction, prior relationship quality, and current relationship quality), were identified to have positive relationships with subjective wellbeing. The presence of these associations form some support for the Stress Process Model, in that factors relating to caregiving outcomes have included variables from both the stressor and mediator levels. However, to provide further support for the theory, additional research is required to determine if these factors are causal to wellbeing outcomes.
Although the present study cannot determine causation, the positive and negative associations found provide some interesting implications for this population of caregivers. Firstly, the negative association between sleep and wellbeing scores indicates that caregivers who reported frequent sleep disruptions were likely to report lower wellbeing scores. This relationship is consistent with previous literature, which has seen sleep disruptions and deprivation to be strongly associated with poorer physical and psychological health outcomes, including increased risk of mortality24.
More positively, three of the mediating variables were identified to have positive relationships with subjective wellbeing, which may have implications to reduce negative outcomes in this population. The first of these variables was caregiving satisfaction; this indicated persons who report higher satisfaction in caregiving were likely to report their subjective wellbeing highly. In addition, both the relationship quality variables had positive associations with subjective wellbeing. This is indicative that persons with higher perceptions of relationship quality with the recipient of their care are likely also to have higher subjective wellbeing. Granted, the data across the relationship quality variables were negatively skewed, displaying most of the caregivers rated the quality of their relationship both prior to the wound and at current, towards the high end of the scale. Nevertheless, the presence of these relationships indicates it is possible interventions to bolster relationship quality and caregiving satisfaction may improve caregiver outcomes within this population.
Interestingly, a number of the predictor variables were associated with one another within this sample. Positive associations were found between relationship quality variables and caregiving satisfaction. This was indicative that persons who perceived the relationship quality as high were likely to report higher satisfaction in the role. The significance of current perceived relationship quality’s correlation with caregiving satisfaction was consistent with the literature. In a prior study investigating informal caregivers of dependent elderly, perceived relationship quality was found to influence caregiving satisfaction22.
In addition, a positive association was found between the two relationship quality variables, indicating if they perceived their relationship to have high quality prior to the wound, they were likely to also rate their relationship highly at the time of testing. Alternatively, the finding in the present study may have been confounded by the nature of the question. The participants were asked to reflect on the quality of the relationship prior to the wound, rather than prior to caregiving. As 47.4% of the sample were providing care prior to the wound, it is possible that the wound was an additional stressor on an existing caregiving role, and did not substantially influence the perceptions of the relationship. Due to this, the literature could benefit from longitudinal research into these factors, perhaps across persons at high risk of developing wounds.
Limitations
Several limitations were identified amongst the present study. Convenience sampling was employed due to the time-pressed nature of the research and the hard-to-reach population investigated. It has been suggested previously that convenience sampling from formal care facilitates may lead to overrepresentations of caregiver burden19. Therefore, it is possible the sample was not fully representative of the true parameters of subjective wellbeing amongst people informally caring for people with wounds. However, this suggestion was likely on the basis of the majority of caregiver research, which has typically addressed the informal caregivers of people with dementia19. Considering this, the reasons for seeking formal care when a person is caring for someone with cognitive decline are likely to be different to a person with a wound. This may especially be a factor in wounds caused by a pre-existing condition such as diabetes, where risk of amputation is high without early intervention25. Therefore, these results should not be generalised to all persons caring for someone with a wound, and should be used as a basis for further research.
Implications
Despite the abovementioned limitations, little research had investigated the effects of informal caregiving amongst the caregivers of people with wounds2,12. In particular, implications of the role had not been measured quantitatively amongst this population previously, nor had relationships between these variables been established prior. Due to this, the present study provided additional insights into the experiences of this population of informal caregivers, and suggests several implications for future research. As previous literature has established, the outcomes of the caregiver may be influenced by the condition of the care recipient and the evidence of co-morbidity within the present sample, it is possible the type of wound may be equally influential26. As such, future studies should investigate the differences in both outcomes, and challenges faced by the caregivers of people living with different types of wounds. The additions of the proposed research may not only provide supplementary insights into the complexity of the factors influencing caregiver outcomes, but also identify if higher incidences of burden are present across certain populations of informal caregivers.
Conclusion
To conclude, the present study implied that subjective wellbeing scores are lower amongst the informal caregivers of people with wounds than the general population of Australians. Several factors correlate with subjective wellbeing, and can be identified as possible stressors and mediators in accordance with the Stress Process Model. These factors include: sleep, relationship quality and caregiving satisfaction. These findings contribute to the existing wound care literature, and provided indication for future research, specifically into the effects of wound type, and causal factors contributing to caregiving outcomes.
Acknowledgements
The following project was conducted with the support and assistance of persons employed by ACT Health hospitals and community health centres. No conflicts of interests were present throughout the duration of this project. We thank the staff, patients and carers for their support with this study. In particular, we wish to extend our thanks to Judith Barker, who assisted with the recruitment of participants.
Author(s)
Katherine Rich*
BScPsych (Hons)
School of Applied Psychology
University of Canberra, ACT 2601, Australia
Email katherine.rich@uni.canberra.edu.au
Dominic Upton
PhD, FBPsS
Acting Dean Education, University of Canberra, ACT 2601, Australia
Email dominic.upton@canberra.edu.au
* Corresponding author
References
- Australian Wound Management Association (AWMA). Wound Awareness Week Resources; 2015. Available from: http://www.awma.com.au/pages/experts.php.
- Upton D, Upton P, Alexander R. The complexity of caring (Part 1): Detrimental health and well-being outcomes for caregivers of people with chronic wounds. Wound Practice & Research 2015a;23:104–8.
- Upton D, Upton P, Alexander R. Well-being in wounds inventory (WOWI): Development of a valid and reliable measure of well-being in patients with wounds. J Wound Care 2016;25:114–20.
- Marino JB. Emotional impact on familial caregivers of the diabetic foot ulcer patient. The Foot 2013;23:111–2.
- Upton D, Andrews A, Upton P. Venous leg ulcers: What about well-being. J Wound Care 2014;23:14–7.
- Millar C, Kapp S. Informal carers and wound management: An integrative literature review. J Wound Care 2015;24:489–97.
- Carretero S, Garcés J, Ródenas F, Sanjosé V. The informal caregiver’s burden of dependent people: Theory and empirical review. Arch Gerontol Geriatr 2009;49:74–9.
- Joseph S, Becker S, Elwick H, Silburn R. Adult carers quality of life questionnaire (AC-QoL): development of an evidence-based tool. Ment Health Rev 2012;17:57–69.
- Bolas H, Van Wersch A, Flynn D. The well-being of young people who care for a dependent relative: An interpretative phenomenological analysis. Psychol Health 2007;22:829–50.
- Brown M, Brown SL. Informal Caregiving: A Reappraisal of Effects on Caregivers. Soc Issues Policy Rev 2014;8(1):74–104.
- Van den Berg B, Fiebig DG, Hall J. Well-being loses due to care-giving. Eur J Health Econ 2014;35:123–31.
- Upton D, Upton P, Alexander R. The complexity of caring (Part 2): Moderators of detrimental health and well-being outcomes for caregivers of people with chronic wounds. Wound Practice & Research 2015b;23:110–4.
- Cummins RA. Subjective wellbeing, homeostatically protected mood and depression: A synthesis. J Happiness Stud 2010;11:1–17.
- Richardson B, Fuller Tyszkiewicz MD, Tomyn AJ, Cummins RA. The psychometric equivalence of the Personal Wellbeing Index for normally functioning and homeostatically defeated Australian adults. J Happiness Stud 2016;17:627–41.
- Hammond T, Weinberg MK, Cummins R. The dyadic interaction of relationships and disability type on informal carer subjective well-being. Qual Life Res 2014;23:1535–42.
- Boerner K, Schulz R, Horowitz A. Positive aspects of caregiving and adaption to bereavement. Psychology & Aging 2004;19:668–75.
- Pearlin LI, Mullan JT, Semple SJ, Skaff MM. Caregiving and the stress process: An overview of concepts and their measures. The Gerontologist 1990;30:583–94.
- Shirai Y, Koerner SS, Kenyon DY. Reaping caregiver feelings of gain: The roles of socio-emotional support and mastery. Aging & Mental Health 2009;13:106–17.
- Tuithof M, ten Have M, van Dorsselaer S, de Graaf R. Emotional disorders among informal caregivers in the general population: Target groups for prevention. Bio Med Central Psychiatry 2015;15:23–31.
- Pearlin LI, Menaghan EG, Lieberman MA, Mullan JT. The stress process model. J Health Soc Behav 1981;22:337–56.
- Lawton MP, Moss M, Hoffman C, Perkinson M. Two transitions in daughters’ caregiving careers. The Gerontologist 2000;40:437–48.
- López J, López-Arrieta JJ, Crespo M. Factors associated with positive impact of caring for elderly and dependant relatives. Arch Gerontol Geriatr 2005;41:81–94.
- Group IW. Personal Wellbeing Index: 5th Edn. Melbourne: Australian Centre on Quality of Life, Deakin University; 2013.
- Arber S, Venn S. Caregiving at night: Understanding the impact on carers. J Aging Stud 2011;24:155–65.
- Hinchliffe RJ. Amputations in patients with diabetes. Br J Surg 2011;98:1679–81.
- Kim Y, Schulz R. Family caregivers’ strains: comparative analysis of cancer caregiving with dementia, diabetes, and frail elderly caregiving. J Aging Health 2008;20:483–503.

