

Volume 40 Number 3
Successful treatment of an ileal conduit fistula with negative pressure: report of a case
Mengxiao Jiang, Huiming Lu, Meichun Zheng, Baojia Luo and Huiying Qin
Keywords negative pressure, dual tube, fistula of ileal conduit, urostomy
For referencing Jiang M et al. Successful treatment of an ileal conduit fistula with negative pressure: report of a case. WCET® Journal 2020;40(3):19-23.
DOI https://doi.org/10.33235/wcet.40.3.19-23
Abstract
Aim To present the management of a patient who developed a fistula from a uretero-ileostomy anastomosis of the ileal conduit by applying intra-conduit negative pressure through a dual tube.
Case report The patient was a 73-year-old man diagnosed with bladder cancer who underwent a radical cystectomy and formation of an ileal conduit in our centre. A fistula occurred in the ileal conduit less than 1 week after the surgery. Urine leaked continuously into the pelvic cavity which put the patient at risk of fluid and electrolyte imbalances. A further operation to suture the fistula to contain the leakage was suggested. To save the patient from a further operation, intra-conduit negative pressure through a dual tube was attempted to assist with management of the fistula. This conservative treatment promoted successful closure of the fistula.
Method It is clinically challenging to manage a urinary fistula associated with an ileal conduit in a conservative way. This is because the fistula is deep within the body cavity and it is almost impossible for the fistula to heal spontaneously. The literature reveals previous conservative treatment has been mostly unsuccessful. Surgical suturing of the fistula is the most used method but is not always an ideal choice. By applying intra-conduit negative pressure through a dual tube system to the ileal conduit, the aim was to facilitate closure of the fistula.
Conclusion In this case report the application of intra-conduit negative pressure through a dual tube to contain a fistula from a uretero-ileostomy anastomosis of an ileal conduit was found to be safe and effective. This method of conservative treatment is worth promoting.
Introduction
Bladder cancer is a highly prevalent disease associated with high recurrence and mortality1. Radical cystectomy is the gold standard treatment for both muscle invasive bladder cancer and recurrent high grade non-muscle invasive bladder cancer2. After radical cystectomy, surgeons mostly choose the formation of an ileal conduit or urostomy for urinary diversion3. It is reported that 15–16% of patients will develop a fistula within the conduit after urinary diversion4,5. Urinary fistula of an ileal conduit is a complex and serious complication that often occurs in the early postoperative period2,5. The occurrence of this complication will not only prolong the hospital stay of patients, but also increases the mortality rate5.
Management of a urinary fistula within an ileal conduit is difficult6. One management option to deal with this complication is further surgery to suture the fistula; however, operating twice on the patient in a short time can cause too much trauma. Doctors and ET nurses often feel very conflicted as to whether to operate a second time, especially when a patient’s physical and psychological condition may not be robust enough to tolerate secondary surgery. Further, the patient may refuse a second operation. In addition to surgical treatment, the literature reveals that other conservative management strategies such as percutaneous nephrostomy or a fenestrated conduit catheter usually fail to close the fistula5.
Negative pressure therapy is widely used to treat fistulas as it facilitates and accelerates drainage of fluid which increases the likelihood of the fistula healing7–9. Through a literature review, the authors found positive results in several patients with a fistula of an ileal conduit following the application of negative pressure therapy10,11. While these previous studies revealed that negative pressure therapy maybe a good clinical choice for managing a urinary fistula within an ileal conduit, these relevant reports are too few and more studies are needed to confirm the safety and efficacy of the treatment. Moreover, clinicians must be aware that ileal conduits are very vulnerable to secondary trauma during the negative therapy processes from the amount of negative pressure applied and catheter-related damage to the conduit5. In this case report, the authors present the outcome of the application of intra-conduit negative pressure in a patient with a fistula in a uretero-ileostomy anastomosis of an ileal conduit. The authors further demonstrate how to use a dual tube to decrease the treatment risk.
Case Presentation
A 73-year-old man in otherwise good health underwent a radical cystectomy and formation of an ileal conduit for muscle invasive bladder cancer. On the 5th postoperative day, the left pelvic drainage tube drained out 1350ml of faint yellow drainage, while the urinary stoma only drained out 700ml of urine. Urinary leakage of the intra-abdominal portion of the ileal conduit was suspected. Examination of fluid from the left pelvic drain confirmed the suspicion and presence of urine as creatinine was confirmed. The level of creatinine present in the drainage fluid was high at 4396.μmol/L – normal range of serum creatinine is 60–110μmol/L. A CT scan of the abdomen showed the fistula was located where the right transplanted ureter entered the ileal conduit.
Careful examination of the ileal conduit was also undertaken and a large amount of mucus was found to have accumulated in the ileal conduit. The doctor flushed the ileal conduit to clear the mucus away. However, although the ileal conduit was no longer obstructed from mucus, the urine still leaked into the pelvic cavity continuously. On the 6th postoperative day, the left pelvic drainage increased to 1890ml, while the urine draining out from the stoma decreased to 410ml. Urine leakage increased the risk of pelvic infection and water electrolyte imbalance; both clinical problems needed to be managed properly as soon as possible. A further operation to suture the fistula closed was suggested. However, taking the trauma of further surgery, the economic cost and the patient’s will into consideration, it was decided to attempt implementation of conservative treatment first.
Negative pressure therapy
The negative pressure system used was constructed by a doctor and an ET nurse. The authors chose this therapy with the aim of achieving two goals. Firstly to stop urine draining continuously into the pelvic cavity and secondly to promote the closure of fistula. A well-known contraindication is to apply negative pressure therapy to organs because the risk of traumatising organs is high. To avoid adverse events such as bleeding, ischaemia and catheter-related ileal conduit perforation from happening, the authors applied negative pressure to the ileal conduit through a dual tube (Figure 1). The dual tube consisted of a rigid tube and a soft tube. The rigid tube could conduct negative pressure well; however, it may cause mechanical damage to the ileal conduit. The soft tube was unable to sustain negative pressure but could protect the ileal conduit from catheter-related injuries by isolating the rigid tube from coming into contact with the ileal conduit. The steps used to construct and apply the therapeutic negative pressure system are listed as follows.
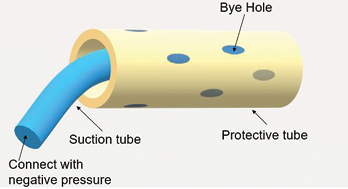
Figure 1. An illustration of a dual tube
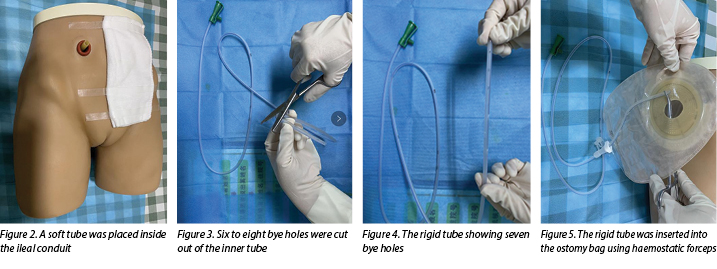
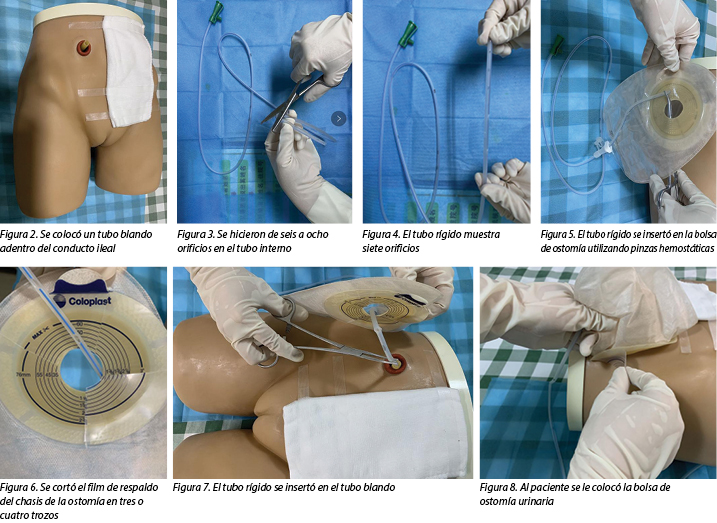
- Select a soft and protective medical latex tube as the outer tube. A soft tube is routinely placed inside the ileal conduit during operation and, as this tube had not been removed when the urinary fistula occurred in our case, it was used as the outer tube (Figure 2).
- Select a rigid tube such as a medical sputum aspiration tube as the inner tube.
- Cut six to eight bye holes out of the inner tube (Figures 3–4).
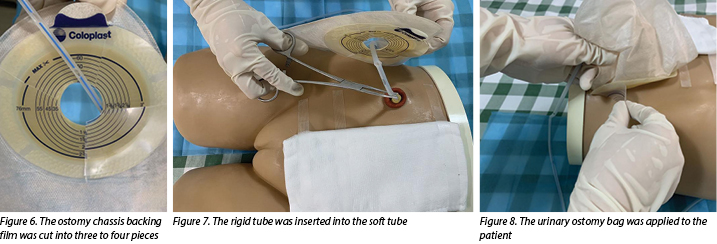
- Insert the rigid tube into the ostomy bag with haemostatic forceps (Figure 5), cut the ostomy chassis backing film into three to four pieces(Figure 6).
- The doctor then inserts a rigid tube into the soft tube (Figure 7). The insertion depth of the inner tube should be 1cm shorter than the outer tube.
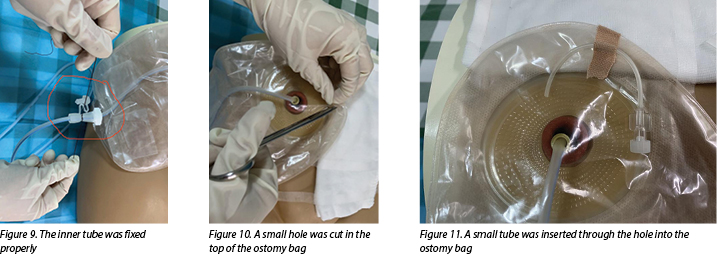
- Apply a urinary ostomy bag to the ostomy skin barrier or base plate (Figure 8) and fix the inner tube properly (Figure 9).
- Cut a small hole in the top of the ostomy bag (Figure 10), and insert a small tube through the hole into the ostomy bag to make the negative pressure semi-closed (Figure 11).
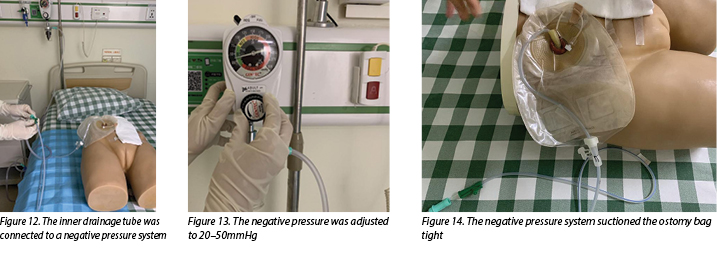
- Connect the inner drainage tube to a negative pressure system (Figure 12) and adjust the negative pressure to 20–50mmHg (Figure 13). In this case, wall suction was used, but a commercial negative pressure therapy machine is also suggested.
- After doing this, observe the negative pressure system suctioning the ostomy bag tight and, at the same time, urine should be immediately sucked out from the ileal conduit (Figure 14).
During the negative pressure therapy process, the patient’s fluid and electrolyte balance was closely monitored, the ileal conduit was cleared of mucus twice a day, and the patient was instructed to do passive activities while in bed. A nutritionist and psychotherapist were invited to join the medical, ET and nursing team to help improve the nutritional and psychological status of the patient.
After 12 days of negative pressure therapy treatment, the left pelvic drainage decreased to 210ml and the creatinine level of the drainage output was 73.7μmol/L, which indicated that urine was no longer leaking into the pelvic cavity. The negative pressure therapy was stopped 2 days later. It was pleasing to note that, following cessation of suction of the urine, there was no increase in pelvic drainage. The patient recovered well and was discharged from the hospital soon after. After a follow-up period of 3 months, no further anastomotic insufficiency was noted.
Discussion
While not a medical emergency, a fistula within an ileal conduit is a complication that is very difficult to manage conservatively. Up till now, the treatment of this type of fistula occurrence has still been in exploratory stages. Conservative management strategies such as percutaneous nephrostomy and fenestrated conduit catheters have been tried to manage these situations, but are reported to have a high failure rate5. Percutaneous nephrostomies are commonly used for urinary diversion, resulting in successful drainage of urine12; however, this method of urinary diversion does not aid fistula healing. Similarly, placing a fenestrated drainage tube or fenestrated catheter into an ileal conduit is also ineffective. While this method may increase the patency of urine drainage it does not prevent urine from leaking into the pelvic cavity, nor does it promote development of granulation tissue around the fistula to assist with fistula closure.
Proper drainage of urine and promotion of the growth of granulation tissue are keys factors for healing fistulas of this nature. Negative pressure systems can help stimulate the formation of granulation tissue and remove excess exudate away from the wound site13. Thus, negative pressure therapy may be a useful alternative for the treatment of urinary fistula. Continuous suction leads to the absorption of leaking urine and intestinal mucus that can cause infection and disturb fluid and electrolyte balance of the patient. In addition, stimulation of angiogenesis and granulation tissue formation increases the chance of fistula healing.
Although negative pressure appears to work well in promoting the closure of fistulas, it should be used and applied with caution to fistulas within an ileal conduit. Adverse events such as bleeding, ischaemia and intestinal perforation may occur due to using negative pressure therapy to exposed organs14. Safety is more important than a curative effect. Although no adverse events have been reported in previous studies10,11,15, this does not mean the therapy is safe and without risk. Some measures must be taken to decrease the treatment risk for the patient. Inserting a protective disc over the exposed organs could offer protection from local ischaemia, while still providing effective drainage16.
In the dual tube model discussed here, the outer tube acted as a protective disc, thereby protecting the ileal conduit from mechanical injury and decreasing the risk of ischaemia and haemorrhage that may be caused by negative pressure. An animal experiment showed negative pressure between 50–170mmHg caused a significant decrease in the microvascular blood flow in the intestinal loops16. The authors, therefore, adjusted the negative pressure to 20–50mmHg in this case to avoid ischaemia occurring. Compared with intestinal fistula, it was less likely that the suction tube would be obstructed when in a urinary fistula, so there was less need to adjust the negative pressure to more than 50mmHg. Moreover, keeping the negative pressure semi-closed was also a protective method to avoid ischaemia by stopping the tube from being tightly suctioned to intestinal tissue for long periods.
There are currently very few recommendations on the use of negative pressure therapy for the management of urinary fistula. As the patient did not have coagulation defects, the authors felt that, under close clinical observation, it would be worth trying very gentle negative pressure through a dual tube approach to aid urinary fistula healing. During the therapy process, it is necessary to regularly check whether the suction tube is displaced or obstructed, monitor the amount of the pelvic drainage and urine discharged in the collecting system of the device daily, and be alert for complications such as bleeding, ischaemia, infection and fluid and electrolyte imbalances. Urinary leakage at the anastomotic site of an ileal conduit can lead to periureteral fibrosis and scarring, thus predisposing to stricture formation6. Surgical follow-up to evaluate anastomotic status is also needed.
Summary
Fistula occurrence at the site of an ileal conduit is a serious complication after urostomy formation. How to promote the closure of urinary fistula quickly and effectively in a conservative way has been problematic and concerning for urologists and ET nurses for a long time. In this case report the authors have shared their successful experience with the application of negative pressure through a dual tube system to manage this complication. The treatment in this instance was found to be safe and effective. It is worth further exploration as the authors believe more patients could benefit from it.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
The authors received no funding for this study.
Tratamiento con éxito de una fístula del conducto ileal con presión negativa: informe de un caso
Mengxiao Jiang, Huiming Lu, Meichun Zheng, Baojia Luo and Huiying Qin
DOI: https://doi.org/10.33235/wcet.40.3.19-23
Resumen
Objetivo Presentar el tratamiento de un paciente al que se le formó una fístula a partir de una anastomosis ureteroileostómica del conducto ileal aplicando presión negativa intraconducto a través de un tubo doble.
Informe de caso El paciente tenía 73 años y un diagnóstico de cáncer de vejiga; fue sometido a una cistectomía radical y se le realizó un conducto ileal en nuestro centro. Le apareció una fístula en el conducto ileal a menos de una semana de haber sido sometido a la cirugía. La orina se filtraba de manera continua a la cavidad pélvica, lo que puso al paciente en riesgo de tener desequilibrios de líquidos y electrolitos. Se sugirió llevar a cabo otra operación para suturar la fístula a fin de contener la pérdida. Para no someter al paciente a otra operación, se intentó una presión negativa intraconducto mediante un tubo doble para asistirlo con el tratamiento de la fístula. Este tratamiento conservador logró el cierre exitoso de la fístula.
Método Es un reto clínico tratar una fístula urinaria asociada con un conducto ileal de manera conservadora. Esto se debe a que la fístula se encuentra en un lugar profundo de la cavidad corporal y a que es casi imposible que la fístula cicatrice de manera espontánea. La bibliografía dice que un tratamiento conservador anterior no había tenido mucho éxito. La sutura quirúrgica de la fístula es el método más utilizado, pero no siempre es la elección ideal. El objetivo era facilitar el cierre de la fístula mediante la aplicación de una presión negativa intraconducto a través de un sistema de tubo doble al conducto íleo.
Conclusión En este informe de caso, se descubrió que la aplicación de presión negativa intraconducto a través de un tubo doble para contener una fístula de una anastomosis ureteroileostómica del conducto ileal es segura y eficaz. Vale la pena incentivar este método de tratamiento conservador.
Introducción
El cáncer de vejiga es una enfermedad altamente prevalente asociada con la alta recurrencia y la mortalidad.1 La cistectomía radical es el tratamiento de referencia tanto para el cáncer de vejiga que invade el músculo como para el cáncer de vejiga recurrente de alto grado que no invade el músculo.2 Después de una cistectomía radical, la mayoría de los cirujanos eligen realizar un conducto ileal o urostomía para el desvío urinario.3 Se informa que un 15–16 % de los pacientes desarrollarán una fístula dentro del conducto después del desvío urinario.4,5 La fístula urinaria de un conducto ileal es una complicación grave y compleja, que a menudo se produce al principio del posoperatorio.2,5 La ocurrencia de esta complicación no solo prolongará la hospitalización de los pacientes, sino también el aumento del índice de mortalidad.5
Resulta difícil realizar el tratamiento de una fístula urinaria dentro de un conducto ileal.6 Una opción de tratamiento para manejar esta complicación es realizar otra cirugía para suturar la fístula; sin embargo, operar dos veces a un paciente en un período breve puede provocar una situación demasiado traumática. Los médicos y el personal de enfermería especializado en TE a menudo sienten un gran conflicto con respecto a [la decisión] de operar una segunda vez, especialmente cuando la condición psicológica y física del paciente puede no ser lo suficientemente fuerte como para tolerar una segunda intervención. Aún más, el paciente puede rehusarse a una segunda cirugía. Además del tratamiento quirúrgico, la bibliografía indica que las otras estrategias de tratamiento conservador, tales como una nefrostomía percutánea o un catéter fenestrado de conducto generalmente no cierra la fístula.5
La terapia de presión negativa se utiliza generalmente para tratar las fístulas, dado que facilita y acelera el drenaje del líquido, lo que aumenta la probabilidad de cicatrizar la fístula.7–9 Mediante la revisión sistemática de la bibliografía, los autores descubrieron resultados positivos después de la aplicación de una terapia de presión negativa a varios pacientes con una fístula en un conducto ileal.10,11 Si bien estos estudios anteriores demostraron que la terapia de presión negativa podría ser una buena elección clínica para tratar una fístula urinaria dentro del conducto ileal, estos informes pertinentes son demasiado escasos y se necesitan más estudios para confirmar la seguridad y la eficacia del tratamiento. Además, los médicos deben ser conscientes de que los conductos ileales son muy vulnerables al trauma secundario durante los procesos de terapia negativa, dada la cantidad de presión negativa aplicada y el daño producido por el catéter al conducto.5 En este informe de caso, los autores presentan el resultado de la aplicación de presión negativa intraconducto en un paciente con una fístula en una anastomosis ureteroileostómica de un conducto ileal. Además los autores demuestran cómo utilizar un tubo doble para disminuir el riesgo del tratamiento.
Presentación del caso
Un hombre de 73 años que, hasta ese momento gozaba de buena salud, se sometió a una cistectomía radical y a la realización de un conducto ileal debido a un cáncer de vejiga que invadía el músculo. Al quinto día del posoperatorio, el tubo del drenaje pélvico izquierdo drenó 1350 ml de un drenaje amarillo pálido, mientras que el estoma urinario solo drenó 700 ml de orina. Se sospechó la existencia de una filtración urinaria de la porción intraabdominal del conducto ileal. El análisis del líquido del drenaje pélvico izquierdo confirmó la sospecha y la presencia de orina como creatinina. El nivel de creatinina presente en el líquido del drenaje era elevado, un 4396 μmol/L, el rango normal de creatinina sérica es 60–110 μmol/L. Una tomografía computada de abdomen mostró que la fístula estaba ubicada donde el uréter derecho trasplantado entraba en el conducto ileal.
También se llevó a cabo una cuidadosa revisación del conducto ileal y se encontró que en dicho conducto se había acumulado una gran cantidad de mucosidad. El médico lavó el conducto ileal para eliminar la mucosidad. Sin embargo, a pesar de que el conducto ileal ya no estaba obstruido con mucosidad, la orina aún se filtraba continuamente a la cavidad pélvica. Al sexto día del posoperatorio, el drenaje pélvico izquierdo aumentó a 1890 ml, mientras que la orina que drenaba del estoma disminuyó a 410 ml. La filtración de orina aumentó el riesgo de infección pélvica y de desequilibrio hidroelectrolítico. Se debían tratar ambos problemas clínicos tan pronto como fuera posible. Se sugirió llevar a cabo otra operación para cerrar la fístula. Sin embargo, teniendo en cuenta el trauma de otra cirugía, el coste económico y al paciente, se decidió implementar primero un tratamiento conservador.
Terapia de presión negativa
El sistema de presión negativa utilizado fue desarrollado por un médico y por el personal de enfermería especializado en TE. Los autores eligieron esta terapia a fin de lograr dos nuevas metas. En primer lugar, detener el permanente drenaje de orina a la cavidad pélvica y, en segundo lugar, favorecer el cierre de la fístula. Una contraindicación bien conocida es aplicar terapia de presión negativa en los órganos debido al alto riesgo de producirles un trauma. Para evitar que sucedan estos eventos adversos, tales como sangrado, isquemia y perforación del conducto ileal relacionado con el catéter, los autores aplicaron presión negativa al conducto ileal a través de un tubo doble (Figura 1). El tubo doble consistía en un tubo rígido y un tubo blando. El tubo rígido podría conducir bien la presión negativa; sin embargo, dicho tubo puede provocar un daño mecánico al conducto ileal. El tubo blando no pudo sostener la presión negativa, pero pudo proteger al conducto ileal de lesiones relacionadas con el catéter, evitando que el tubo rígido entre en contacto con el conducto ileal. A continuación, se enumeran los pasos seguidos para desarrollar y aplicar el sistema de presión negativa terapéutica.
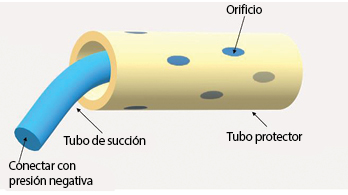
Figura 1. Una ilustración de un tubo doble
- Seleccionar un tubo protector blando de látex de uso médico como tubo externo. Como rutina se coloca un tubo blando adentro del conducto ileal durante la operación y, como en nuestro caso este tubo no se había quitado cuando apareció la fístula, se utilizó como tubo externo (Figura 2).
- Seleccionar un tubo rígido, tal como un tubo de uso médico de aspiración mucolítica, como tubo interno.
- Realizar de seis a ocho orificios en el tubo interno (Figuras 3–4).
- Insertar el tubo rígido en la bolsa de ostomía con pinzas hemostáticas (Figura 5), cortar el film de respaldo del chasis de la ostomía en tres o cuatro trozos (Figura 6).
- Luego, el médico inserta un tubo rígidodentro de un tubo blando (Figura 7). La profundidad de la inserción del tubo interno debe ser 1 cm más corta que la del tubo externo.
- Colocar una bolsa de ostomía urinaria a la barrera de la piel de ostomía o a la placa de base (Figura 8) y colocar el tubo interno adecuadamente (Figura 9).
- Hacer un pequeño orificio en el borde superior de la bolsa de ostomía (Figura 10) e insertar un tubo pequeño a través del orificio de dicha bolsa para lograr que la presión negativa sea semicerrada (Figura 11).
- Conectar el tubo de drenaje interno a un sistema de presión negativa (Figura 12) y regular la presión negativa a 20–50 mmHg (Figura 13). En este caso, se utilizó una succión de pared, pero también se sugiere una máquina comercial de terapia de presión negativa.
- Después de hacer esto, prestar atención a que el sistema de presión negativa succione la bolsa de ostomía bien cerrada y que, al mismo tiempo, la orina se succione de inmediato del conducto ileal (Figura 14).

Durante el proceso de terapia de presión negativa, se monitoreó estrechamente el equilibrio del líquido y los electrolitos del paciente, se limpió el conducto ileal de mucosidad dos veces por día y se instruyó al paciente para que hiciera actividades pasivas mientras estuviera en cama. Un(a) nutricionista y un(a) psicoterapeuta fueron invitados a unirse al equipo médico, al de TE y al de enfermería para ayudar a mejorar el estado nutricional y psicológico del paciente.
Después de 12 días de tratamiento con terapia de presión negativa, el drenaje pélvico izquierdo disminuyó a 210 ml y el nivel de creatinina de la salida del drenaje era de 73,7 μmol/L, lo que indicaba que la orina ya no se filtraba más a la cavidad pélvica. Dos días más tarde se suspendió la terapia de presión negativa. Fue grato observar que, después de detener la aspiración de la orina, no hubo aumento en el drenaje pélvico. El paciente se recuperó bien y se le dio el alta del hospital poco después. Después de un período de seguimiento de tres meses, no se observó insuficiencia anastómotica.
Discusión
Si bien no es una urgencia médica, una fístula dentro de un conducto ileal es una complicación muy difícil de tratar de manera conservadora. Hasta ahora, el tratamiento para este tipo de formación de fístula se encuentra aún en etapa exploratoria. Se han tratado estrategias de tratamiento conservador, tales como la nefrostomía percutánea y los catéteres fenestrados de conducto para tratar estas situaciones, pero el informe indica que hay un alto índice de fracasos.5 Las nefrostomías percutáneas se utilizan comúnmente para la desviación urinaria, que da como resultado un drenaje de orina exitoso12; sin embargo, este método de desviación urinaria no ayuda a cicatrizar la fístula. De la misma manera que tampoco resulta eficaz colocar un tubo de drenaje fenestrado o un catéter fenestrado dentro un conducto ileal. Si bien este método puede aumentar la permeabilidad del drenaje de orina, no evita que la orina se filtre a la cavidad pélvica, ni tampoco favorece el desarrollo del tejido de granulación alrededor de la fístula para ayudar al cierre de la misma.
El drenaje de orina adecuado y el favorecimiento del crecimiento del tejido de granulación son factores clave para la cicatrización de las fístulas de esta naturaleza. Los sistemas de presión negativa pueden ayudar a estimular la formación del tejido de granulación y a eliminar el exceso de exudado del sitio de la herida.13 Por consiguiente, la terapia de presión negativa puede ser una alternativa útil para el tratamiento de la fístula urinaria. La aspiración continua hace que se absorba la orina y la mucosidad intestinal, que pueden provocar una infección y perturbar el equilibrio del líquido y de los electrolitos del paciente. Además, la estimulación de la angiogénesis y la formación del tejido de granulación aumentan la posibilidad de cicatrización de la fístula.
A pesar de que la presión negativa parece funcionar bien para favorecer el cierre de las fístulas, se debe utilizar y aplicar con precaución a las fístulas que se encuentran dentro de un conducto ileal. Pueden ocurrir eventos adversos, tales como sangrado, isquemia y perforación intestinal debido al uso de terapia de presión negativa a órganos expuestos.14 La seguridad es más importante que un efecto curativo. A pesar de que no se han informado eventos adversos en estudios anteriores10,11,15, esto no implica que la terapia sea segura y que no tenga riesgos. Se deben tomar algunas medidas para disminuir el riesgo del tratamiento para el paciente. La inserción de un disco protector sobre los órganos expuestos podría evitar que se produzca una isquemia local, a la vez que también brinda un drenaje eficaz.16
En el modelo de tubo doble que se debate aquí, el tubo externo actuó como disco protector; es decir, protegiendo el conducto ileal de una lesión mecánica y disminuyendo el riesgo de isquemia y hemorragia, que pueden ser provocadas por la presión negativa. Un experimento en animales demostró que la presión negativa entre 50–170 mmHg provocó una disminución importante del flujo sanguíneo microvascular en las asas intestinales.16 Por consiguiente, los autores ajustaron la presión negativa a 20–50 mmHg en este caso para evitar que se produzca una isquemia. Comparado con la fístula intestinal, hubo menos probabilidad de que el tubo de succión se obstruyera que en el caso de una fístula urinaria; por lo tanto, hubo menos necesidad de regular la presión negativa a más de 50 mmHg. Además, mantener la presión negativa semicerrada también fue un método protector para evitar la isquemia, impidiendo que el tubo sea fuertemente succionado al tejido intestinal durante largos períodos.
Actualmente, hay muy pocas recomendaciones para el uso de la terapia de presión negativa para el tratamiento de la fístula urinaria. Dado que el paciente no tenía problemas de coagulación, los autores pensaron que, bajo estrecha observación clínica, valdría la pena probar la aplicación de una presión negativa muy suave a través de un tubo doble para ayudar a la cicatrización de la fístula urinaria. Durante el proceso de la terapia, es necesario controlar periódicamente si el tubo de succión está mal colocado u obstruido, monitorear diariamente la cantidad de drenaje pélvico y de orina eliminada en el sistema de recolección del dispositivo, y estar alerta por si hay complicaciones como sangrado, isquemia, infección y desequilibrio de líquidos y electrolitos. La filtración urinaria en el sitio anastomótico de un conducto ileal puede provocar una fibrosis periureteral y dejar cicatrices, por consiguiente, predisponiendo a la formación de una estenosis.6 También es necesario un seguimiento quirúrgico para evaluar el estado anastomótico.
Resumen
La posibilidad de que se forme una fístula en el sitio de un conducto ileal es una complicación grave después de una urostomía. Durante mucho tiempo, a los urólogos y al personal de enfermería especializado en TE les ha resultado problemático y de gran preocupación el tema de cómo favorecer el cierre de la fístula urinaria de manera rápida, eficaz y conservadora. En este informe de caso, los autores han compartido su experiencia exitosa con la aplicación de presión negativa mediante un sistema de tubo doble para tratar esta complicación. Se descubrió que en esta instancia el tratamiento era seguro y eficaz. Vale la pena realizar más estudios, dado que los autores creen que más pacientes podrían beneficiarse de este tratamiento.
Conflicto de intereses
Los autores declaran que no hay conflictos de intereses.
Financiación
Los autores no recibieron financiación para este estudio.
Author(s)
Mengxiao Jiang
MD
Department of Urology Surgery; Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China; Collaborative Innovation Center for Cancer Medicine
Huiming Lu
BD
Department of Urology Surgery; Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China; Collaborative Innovation Center for Cancer Medicine
Meichun Zheng
BD
Department of Colorectal Surgery; Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China; Collaborative Innovation Center for Cancer Medicine
Baojia Luo
MD
Department of Colorectal Surgery; Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China; Collaborative Innovation Center for Cancer Medicine
Huiying Qin*
MD
Department of Nursing Division, Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China; Collaborative Innovation Center for Cancer Medicine
Email qinhy@sysucc.org.cn
* Corresponding author
References
- Sanli O, Dobruch J ,Knowles MA, et al. Bladder cancer. Nat Rev Dis Primers, 2017;3:17022. doi:10.1038/nrdp.2017.22
- Wei ST, Lamb BW, Kelly JD. Complications of radical cystectomy and orthotopic reconstruction. Adv Urol 2015;2015(3):1-7. doi:10.1155/2015/323157.
- Kotb A F. Ileal conduit post radical cystectomy: modifications of the technique. J Ecancermedicalscience 2013;7:301.
- Teixeira SC, Ferenschild FT, Solomon MJ, et al. Urological leaks after pelvic exenterations comparing formation of colonic and ileal conduits. Eur J Surg Oncol 2012;38(4):361–366.
- Brown KG, Koh CE, Vasilaras A, et al. Clinical algorithms for the diagnosis and management of urological leaks following pelvic exenteration. Eur J Surg Oncol 2014;40(6):775–781.
- Farnham SB, Cookson MS. Surgical complications of urinary diversion. World J Urol 2004;22(3):157–167.
- Bobkiewicz A, Walczak D, Smolinski S, et al. Management of enteroatmospheric fistula with negative pressure wound therapy in open abdomen treatment: a multicentre observational study. Int Wound J 2017;14(1):255–264.
- Ruiz-Lopez M, Titos A, Gonzalez-Poveda I, et al. Negative pressure therapy as palliative treatment for a colonic fistula. Int Wound J 2014;11(2):228–229.
- Loaec E, Vaillant PY, Bonne L, et al. Negative-pressure wound therapy for the treatment of pharyngocutaneous fistula. Eur Ann Otorhinolaryngol Head Neck Dis 2014;131(6):351–355.
- Yetişir F, Salman AE, Aygar M, et al. Management of fistula of ileal conduit in open abdomen by intra-condoit negative pressure system. Int J Surg Case Rep 2014;5(7):385–388.
- Denzinger S, Luebke L, Burger M, et al. Vacuum-assisted closure therapy in ureteroileal anastomotic leakage after surgical therapy of bladder cancer. World J Surg Oncol 2007;5(1):41.
- Ahmad I, Pansota MS. Comparison between double J (DJ) ureteral stenting and percutaneous nephrostomy (PCN) in obstructive uropathy. Pakistan J Med Sci 2013;29(3):725–729.
- Wolvos T. The evolution of negative pressure wound therapy: negative pressure wound therapy with instillation. J Wound Care 2015;24(4 Suppl):15–20.
- Ontario HQ. Negative pressure wound therapy: an evidence update. Ontario Health Technology Assessment 2010;10(22):1.
- Heap S, Mehra S, Tavakoli A, et al. Negative pressure wound therapy used to heal complex urinary fistula wounds following renal transplantation into an ileal conduit. Am J Transplant 2010;10(10):2370–2373.
- Lindstedt S, Hlebowicz J. Blood flow response in small intestinal loops at different depths during negative pressure wound therapy of the open abdomen. Int Wound J 2013;10(4):411–417.

